

Denise Foster Scott is a Certified Advanced Soma Practitioner and has been in practice since 2008 in Washington and Oregon. She is an instructor at the Soma Institute of Neuromuscular Integration® teaching anatomy and physiology as well as core Soma structural integration principles. Denise is also the current Vice-President of IASI. You may reach Denise at [email protected].
Abstract
This article is to report the findings from a single-case research which examined the effects of a once-weekly, eleven series of Soma Structural Integration on a client with pectus excavatum. The intervention lasted approximately eleven weeks. Results indicate that structural integration helped improve structural verticality, chest expansion, and increased adaptive capacity of respiration.
The adjustment of the structure in the thoracic cavity was easily noted visually.
In November of 2010, a then 26-year old Caucasian male named Daryl came to my office seeking improvement for his posture. Daryl has pectus excavatum, an abnormal formation of the ribcage that gives the chest a caved-in or sunken appearance. In 2001, Daryl underwent pectus excavatum repair surgery in an attempt to correct the chest deformity, which was impairing his heart and lung function. The surgery involved removal of costochondral cartilage and reshaping of the sternum. At the time of his first visit with me, Daryl was enjoying overall good health, with none of the respiratory or cardiac issues that plagued him before the surgery. He did note feeling tight in his upper back and hamstrings, decreased flexibility, and he wanted to increase his capacity for exercise. He had also previously been diagnosed with uneven leg lengths. In combination with the pectus excavatum, this caused him to be hunched over for a fair portion of his life.
Daryl had a goal of entering the military to be a guard to the Tomb of the Unknown Soldier in
Arlington National Cemetery. Postural requirements are strict to obtain this honor, with a minimum qualification by the United States Air Force Honor Guard of “no physical disqualifiers, to include history of posture, back, knee, feet, joint or equilibrium problems” (Honor Guard recruiting).
Background
Also known as funnel chest, pectus excavatum is a depression in the sternum. Chest wall disorders typically develop during the formation of the thoracic cavity, which begins in the embryo around the fourth week of gestation with the sternum development in the sixth week (Blanco, 2011). If too much connective tissue that joins the ribs to the sternum in the costochondral region develops, the sternum will defect inward. Pectus excavatum is one of the most common congenital abnormalities of the chest, found in one in every 400 births; it affects men more than women (Canavan, 2008). It is often associated with scoliosis and Marfan syndrome (MedlinePlus), which further suggests that it is a connective tissue disorder (Dugdale & Hadjiliadis, 2011).
Pectus excavatum, if severe, has been known to affect the cardiovascular and respiratory functions in the thoracic cavity. H. A. Kragten reported in the February 2011 Netherlands Heart Journal that seniors with pectus excavatum who were asymptomatic in their youth gradually developed symptomatic conditions by their 40s to 50s. As for Daryl, the symptoms began in his teens. Perhaps as the individual leaves the flexibility of youth, the chest wall begins to stiffen and symptoms develop.
More often though, the disorder is asymptomatic with cosmetic reasons being the driving force behind reconstructive repair. There is a great deal of evidence to support pectus excavatum as a connective tissue disorder. This puts structural integration in a prominent position to work with this condition.
Structural Goals
? Release fascial restrictions of the anterior thorax and diaphragm to allow for chest expansion
? Improve adaptive capacity of respiration and the movement of the three axes of the chest wall
? Balance segments of the body to achieve improved posture
? Align knees and feet
? Increase arch support in feet, reduce bilateral eversion
? Decrease stomach distention (if possible and if structural)
? Improve flexibility
? Improve cardiac/exercise output
Method
The method being used was the Soma Neuromuscular Integration® method of structural integration. Soma is one of the original heirs of Ida P. Rolf ’s Method of structural integration. I followed the standard format for the Soma Structural Integration series with additional emphasis on fascial release of the ribcage to adapt the series to this individual. I also wanted to see improved strength in the diaphragm. Sessions were performed once a week from 11/08/2010 to 01/27/2011.
Soma begins each series with before series photos: anterior, profile, and posterior of the body. We also have our clients do a drawing of themselves. With the instruction to “draw a picture of yourself of how you feel in your body at this moment,” the client is left alone with crayons, pencil and paper for five minutes. This drawing allows the Soma practitioner to learn from the right hemisphere of the brain things that are not readily available through health intake forms and structural analysis, and assists the practitioner with psychosomatic interaction with the client.
Drawing Interpretation
It is clearly evident that Daryl has a dream to achieve. His drawing of his side profile (Figure 1) in the kyphotic stance with the angry face tells me he is unhappy with his posture and believes this may be a deterrent to achieving his goal. I am reminded of Feldenkrais’s statement: “all negative emotion is expressed as flexion” (1949). Daryl’s use of the color black to stand on gives me the sense that there is sadness or depression in his grounding/foundation.
The light blue color on his body I interpreted as a feeling of a personal lack of strength (Bolesky, 2009). The segments of his body were clearly blocky, giving me a clue that the integration sessions would be very important in this series.

Figure 1. Client’s before series drawing of himself.
Postural Analysis
? In the frontal view photograph (Figure 2), I was immediately drawn to the extreme compression in the front of his torso and the pull in the upper thoracic and left shoulder depressing the clavicle. There was an illusion of a long front neck, which was actually a combination of the compression in the thorax and compression in the posterior suboccipitals, which were working to keep the eyes level. There was bilateral anterior rotation of the shoulder girdle and cross-lateral fascial pull from upper left shoulder to lower right hip, which was elevated and rotating posteriorly. The left side of the ribcage was pulling forward, along with the left ilium. The right ilium had a posterior rotation compared to the left and was elevated. Daryl’s head was shifted and being pulled to the right side with the cross-lateral pattern with the right sternocleidomastoid engaged, maybe to counterbalance the rotations below. There was strong engagement of upper trapezius. Also notable was the bilateral lateral rotation of the lower legs, bilateral eversion of the feet (left greater than the right) and flat arches. This much compensation limits complexity of movement, which tends to limit the equipoise of graceful movement.

Figure 2. Before series anterior view

Figure 3. Before series side view

Figure 4. Before posterior view
? In the side profile photograph (Figure 3), the physical evidence that the pectus excavatum has had on his structure is clearly evident. His anterior chest wall is difficult to see due to the indentation of the sternum as well as the bilateral anterior rotation of the shoulder girdle. This mirrors an extreme case of the Upper Crossed Syndrome defined by Vladimir Janda, MD. He summarizes that “Upper Crossed Syndrome is characterized by facilitation of the upper trapezius, levator, sternocleidomastoid, and pectoralis muscles, as well as inhibition of the deep cervical flexors, lower trapezius, and serratus anterior” (n.p.). The distended abdominal region, in my view, is caused by a possible pressure differential occurring between the thoracic and pelvic diaphragms created by the sunken chest.
? The bilateral rounding and anterior rotation, as seen in the posterior view photograph (Figure 4), creates tension in the rhomboids and middle
trapezius. The right sideline was compressed compared to the left allowing a “C” curve to occur in the spine. The anterior cross- lateral strain is reflected in the back with left shoulder elevation and migration forward, right hip elevation. Both legs show medial rotation in the upper thigh with counterbalancing lower leg lateral rotations.
The Sessions Note that the session goals are referenced from Thomas Myers’ article, “Variation in Ida Rolf ’s ‘Recipe’,” from the IASI Yearbook (2004) with the exception of the arm and 10th sessions, which is where Soma differs from the classic 10-session series.
Session 1
Goals: Differentiate the shoulders and ribs; free ribs and sternal restrictions to breathing; begin to shift pelvis to horizontal.
Methods: Traditional session with extra emphasis on hamstrings and thoracic cavity.
Results: There was an immediate improvement of the positioning of the ribcage over the pelvis, expansion of the diaphragm and thoracic cavity. Verticality improved greatly in his structure, with his front line lifting and his torso being supported by a more horizontal pelvis. His head was still contracted at the occipital ridge, and there was still rounding of the shoulders. The distension of his stomach remained unchanged after the session. I took this as a result of the long term exposure to the extreme pressure differentiation between the thoracic and pelvic diaphragms. If one thinks of holding an inflated balloon and then squeezes the top of it, where is the air to go?
Session 2
Goals: Ground the client through feet and establish bilateral support to the spine; balance the arches; lengthen the back erector tissue.
Methods: Traditional session to address bilateral eversion of feet and flat arches. Daryl’s left foot showed more compromise in the supportive structural architecture of the arches. With regards to the extensors in the back, the spine had extreme curves beyond normal. We worked in seated position, and “dug out” the lumbar curve while “piling up” the thoracic curve in an attempt to bring the spine to a more balanced depth. We also addressed additional restrictions that would begin to free up rib articulations at the spine in order to restore proper rib rotation in respiration.
Results: Increased suspension through feet and lower legs and improved forward tracking of feet. Due to the change in gait after session two, Daryl experienced excessive rubbing between toes one and two on the left foot, the push-off point of propulsion (Caspari, 2005). We planned to revisit gait analysis in the third session and hypothesized that the new placement of the foot during gait sequence just needed to acclimate to the new movement pattern.
Session 3
Goals: Lift and lengthen the lateral line from neck to foot; balance the anterior and posterior horizontal relationships; begin the core work via lengthening the quadratus lumborum; free the twelfth ribs.
Methods: Traditional session to address sidelines to balance front and back relationship in the body. We worked to free fascial restriction in the intercostal spaces. We employed client awareness and movement to have Daryl begin to feel the adaptive capacity of respiration and movement of the ribs in all three planes.
Results: The right side lumbodorsal hinge was more compressed, as noted by a spiral fascial contraction from left shoulder to right hip. The fibers of the right quadratus lumborum (QL) at the transverse processes were locked short with adhesions, pulling the twelfth rib downward. We were able to soften the tissue but QL engagement was still evident. The occipital region began to release, allowing the chin to descend into a more neutral position.
Session 4
Goals: Deepen grounding through inner line of leg; open structures attaching to the pelvis from below; differentiate the legs from the pelvis; address the rotation and counter-rotation in the legs.
Methods: Traditional session with adductor and core line releases. Pelvic diaphragm work creating a foundational support for the thoracic diaphragm.
Results: On the left leg, the adductors were engaged with lateral rotation of the lower leg, knee hyperextension, and pelvic floor engaged. The strain engagement in the adductors contributed to the anterior tilt of the pelvis and medial rotation of the upper thigh. Bringing balance to these structures allowed more alignment in the right leg through to the foot, but the left leg remained medially rotated in the upper leg with counter-lateral rotation in the lower leg with everted foot.
Session 5
Goals: Open deep abdominal tissue; release structures attaching to the anterior pelvis; improve the psoas/rectus abdominis relationship.
Methods: Traditional session with employment of a fascia shortening technique on the both the major and minor pectoralis to “unhook” fascia first by moving into the aberrations. Once completed I did cross-lateral fascial release from opposite hip/ opposite shoulder using traction and fascia release techniques.
Results: During the session I found the left psoas more engaged than the right, bringing an anterior tilt to the left ilium. We were able to decrease the cross-lateral strain. Movement of the legs began to be initiated from the psoas. There was more verticality evident with a lift of Daryl’s anterior torso. The posterior rotation in his right ilium eased some and improved thoracic expansion.
Session 6
Goals: Support posterior line from neck to foot. Methods: Traditional session with separating the hamstrings and adductor compartments. Additional attempts to balance the pelvic restrictions in the right side twelfth rib/ilium relationship. Results: The back line was able to lengthen to support the reduced flexion in the front line.
Session 7
Goals: Create new relationship of head segment to pelvis; release deep fascia of neck.
Methods: Traditional session with added pectoralis fascia release to continue to help facilitate the lift in the chest and create availability for the sub-occipitals to relax. I used the same pectoralis and cross-lateral traction techniques as used in session five.
Results: After the session, Daryl’s head was still tilted and shifted to the right, but to a lesser degree. Due to the decrease in the chest compression we had achieved thus far, we were able to release the contraction in the suboccipitals and his chin dropped in response.
Session 8
Goals: Create integration of the lower portion of the body.
Methods: Traditional session with proper joint alignment during movement and applied resistance during activities.
Results: Before the session, the client reported hamstring tightness. After the session, the left ilium was still anterior with medial upper thigh rotation and compensating lateral rotation in the lower leg and eversion of the foot. The capacity of movement through the psoas and improved alignment in gait sequence was beginning to become more natural.
Session 9
Goals: Create integration of the upper portion of the body.
Methods: Traditional session with emphasis on antagonist’s cross-lateral engagement of the posterior torso in opposition to the left shoulder and right hip shortening. With the client prone on the table, I had him feel the cross-lateral connection of the posterior left shoulder to posterior right hip and contract the two together. I had the client do this to make a kinesthetic connection then applied resistance while the client moved to counterbalance and educate movement in that plane.
Results: We achieved integration around the diaphragm. There was still visible pull along the arms into the glenohumeral joint, adding to the rounding of the shoulder girdle.
Arm Session
The Soma series includes an additional integrative session to address arm and shoulder restrictions with movement and joint alignment education.
Goals: Create integration between the head and the counterbalance of the arms (Bolesky, Nolte, & Johnson, 2005).
Methods: Traditional session with release of the superficial and deep fascia of the arms. Integrate the arm and shoulder girdle in relationship to the cranium and torso.
Results: This session proved to be a vital component to obtaining the proper balance of the shoulder girdle on the torso and appropriate counter balance to the head and neck. Before the session, Daryl had bilateral forward tension along the anterior length of his arms. Releasing the fascia of the arms allowed for more balance in the anterior shoulder girdle.
Session 10
Goals: Create integration of entire body and balancing of all joints in gravity.
Methods: In the Soma tradition, this session includes arthrokinetics (AK) which is performed on each joint in an attempt to reset proprioceptive joint positioning. The AK technique brings arrhythmic movements of tension and compression into a joint in all the available angles of the particular joint in question. As described by J.G. Pickard in his article, “Neurophysiological Effects of Spinal Manipulation”:
…biomechanical changes caused by spinal manipulation are thought to have physiological consequences by means of their effects on the inflow of sensory information to the central nervous system. Muscle spindle afferents and Golgi tendon organ afferents are stimulated by spinal manipulation (2002, p. 357).
Although AK can be considered “joint manipulation,” we are by no means performing chiropractic adjustments. AK affects the body’s proprioceptive sense by stimulating Golgi tendon organs—the sensory receptors found in the fibers of tendons that monitor tension in a muscle—allowing the joint to relax into a more neutral position. We use the concepts that movement across the joints affects biomechanical changes.
Results and Overall Conclusions
Looking back at our structural goals listed above, we were able to make progress with all of them, particularly the expansion of the chest and improved verticality of the body. The after photographs are shown below the before photographs in Figure 5 below. The front view photographs show significant expansion and that the “V” positioned clavicles found a horizontal orientation evenly along the chest. More ease was created at the severely shortened, anteriorly rotated left shoulder. The after session photo shows more length in the abdomen and lessening of the extreme curvatures of the spine. The client still had some compression in the chest but this had markedly improved. The distended stomach was still present. The alignment of his right leg improved, while the left was still in less exaggerated counter-rotations. Signs of the elevated right ilium and elevated left shoulder, creating the “C” curve to the spine, indicate to me that there is still cross-lateral integration that needs to be done in the torso.

Figure 5. After series photographs shown below before series photographs.
Ultimately, Daryl was able to increase his cardiac output and enrolled into high intensity training exercise to get into shape for the military. This training improved his posture by strengthening the rhomboids and lower trapezius. However, without the previous structural integration intervention, it is likely that the shoulders would not have been able to stabilize over the ribcage because of the pectoralis fascia restrictions, so his body building exercises would have exaggerated the pectus excavatum with its emphasis on the pectoralis muscles.
After the Series Drawing Interpretation
In conclusion to our series work, Soma practitioners have our clients again draw “how you feel in your body at this moment.” Often times, the before-and-after drawings can be more dramatic than the before-and-after photos. It allows the client to see his emotional shift. For Daryl’s after drawing (Figure 6), it appears that his internal sense is that his body is more vertical and he is a stronger and more whole person able to live his dreams. If you compare the figure in the after drawing to the “dream” drawing in the before drawing, you will see the similarities indicating his dream is becoming a reality.
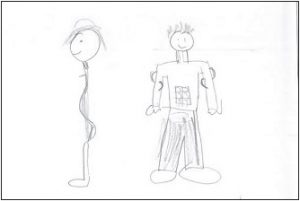
Figure 6. Client’s after series drawing of himself.
Conclusion
Further research is needed to determine the efficacy of structural integration’s intervention on clients with pectus excavatum. Visual structural analysis does support the theory that structural integration can have an effect on clients suffering from pectus excavatum or post-operative pectus excavatum.
On September 27, 2012, I received a note from Daryl with two photos (see Figures 7 and 8). The note said: “Because of working with you, and you helping me open up and stand up straight, I’m working my dream as a Guard of Honor at the Tomb of the Unknown Soldier. Thanks a million!”
— From Arlington National Cemetery.

Figure 7. Daryl achieved his dream of becoming a Guard of Honor.

Figure 8. Daryl marching in front of the Tomb of the Unknown Soldier at Arlington National Cemetery.
Photo by Mark Millich.
A deep, heart-felt thank you to Karen Bolesky for pushing me beyond my boundaries for real growth to occur. To Jennifer Lovejoy, Lanii Chapman, and Breta Stroud for taking the time to proofread this case study.
References
Blanco, F. C., Elliott, S. T., & Sandler, A. D. (2011). Management of congenital chest wall deformities. Seminars in Plastic Surgery, 25(1), 107-116. doi: 10.1055/s-0031-1275177
Bolesky, K. L. (2009). Bony landmarks: Making somatic connections (p. 65). USA: Xlibris.
Bolesky, K. L., Nolte, M., & Johnson, S. W. (2005). Soma neuromuscular integration: how we define ourselves.
In M. Beech (Ed.), IASI 2005 yearbook of structural integration (pp. 14-16). Missoula, MT: International Association of Structural Integrators.
Cahalin, L., & Canavan, P.K. (2008). Integrated physical therapy intervention for a person with pectus excavatum and bilateral shoulder pain: a single-case study. Archives of Physical Medicine and Rehabilitation, 89(11), 2195- 2204. doi: 10.1016/j.apmr.2008.04.014.
Caspari, M. (2005). The functional rationale of the recipe. In M. Beech (Ed.), IASI 2005 yearbook of structural integration (pp. 51-78). Missoula, MT: International Association of Structural Integrators.
Dugdale, D. C., & Hadjiliadis, D. (2011, December 12). Pectus excavatum repair series. Retrieved from Medline Plus: http://www.nlm.nih.gov/medlineplus/ency/ article/003320.htm.
Feldenkrais, M. (1949). Body and mature behavior. New York: International Universities Press.
Honor Guard. http://www.honorguard.af.mil/recruiting Janda, V. Retrieved from http://www.jandaapproach.com/the-janda-approach/jandas-syndromes
Kragten, H. A., Siebenga, J., Höppener, P. F., Verburg, R., & Visker, N. (2011). Symptomatic pectus excavatum in seniors (SPES): a cardiovascular problem?
Netherlands Heart Journal, 19(2),73-78. doi: 10.1007/s12471-010-0067-z
Myers, T. (2004). Variation in Ida Rolf ’s ‘recipe’. In M. Beech (Ed.), IASI yearbook of structural integration (pp. 9-13). Missoula, MT: International Association of Structural Integrators.
Marfan syndrome (n.d.). In MedlinePlus. Retrieved November 18, 2012, from http://www.nlm.nih.gov/ medlineplus/ency/article/000418.htm
Pickard, J. G. (2002). Neurophysiological effects of spinal manipulation. Spinal Journal: Official Journal of the North America Spine Society, 2(5), 357-371.
[:]Pectus Excavatum and Structural Integration: A Case Study