
Foreword
This article describes the development, initially serendipitous, of a style of fascial manipulation currently referred to as Tensegrity Touch. Its outset was the observation from various Rolfer colleagues who noticed “something different” in the my (Bertolucci’s) manipulation maneuvers.
Operating from the Outside: Blunt Dissection
This all started back in the late 1980s, during my residency in physical medicine and rehabilitation. I had planned to study Rolfing® Structural Integration (SI), and by way of illustration to my mentor, I touched his forearm in a way that I described as “freeing the myofascial compartments from each other.” A wise and open-minded orthopedic surgeon, Dr. Rossi added, “You mean that applying Rolfing SI you operate from the outside?” I laughed as if I had heard a joke. Years later this would come back to me, as I will describe below.
I graduated as a Rolfer in 1990 and started my practice in São Paulo. Impressed with the first results of applying Rolfing SI to the same clients to whom I was used to prescribing physiotherapy, I plunged into further study – initially extracellular matrix (ECM) physiology, aiming to better understand what could be happening under a manual therapist’s hands.
A Different Way to Touch?
Around four years later, I started hearing from Rolfer colleagues that my touch felt “somehow different.” As I heard this more and more often, I gathered a group of Rolfers and began an empirical research project to investigate whether there was indeed anything significantly different in the techniques I applied from those traditionally employed in Rolfing SI.
We initially noticed two singular features to my way of working: 1) a way of engaging tissue from the skin that gave the practitioner the clear sense of internal gliding happening under his hands, and 2) a sense of the touch meeting firmness. These were the first of various features progressively identified as components of my style of touch.
One day during a session, I suddenly recalled Dr. Rossi’s words. Sensing internal tissue gliding, I related his words “operating from the outside” to the surgical concept of blunt dissection: a way to separate tissues during an operation using a blunt tool, commonly the fingers. There seemed to be a very precise way to steer one’s touch to the gliding surfaces (planes of cleavage) among myofascial compartments. This led to the nickname of our first workshop: Surgical Rolfing SI.
The main element in achieving this bluntdissection effect seemed to be shearing the skin on top of underlying tissues to the end of its mobility in a particular direction. (We now call it ‘milking’ tissue from one hand to the other.) We surmise this possible biomechanical explanation: shearing tissues further loads the fascial system (beyond its basal prestressed status) to the end of its elastic phase (when the practitioner feels a sudden stop), thus reaching the viscous phase of the tissue in which plastic changes can take place. Such manual loading would tense the matrix links in the superficial fascia (SF) and be transmitted to the remaining matrix ‘net’. As such, the SF could be considered a ‘handle’ to access the fascial system. It is thus as if the practitioner is creating a knife that can reach virtually any location, and the handle of the knife is the loaded tissue in the touch interface.
An abrupt snap (possibly between myofascial compartments) is sometimes noticed during a maneuver, followed by significant clinical improvement. Might the manipulation be affecting relative muscle position (Maas and Sandercock 2010)? This led to another transitory naming attempt, Muscle Repositioning.
Tensegrity Induced by Touch
So we were investigating a way of touching that gave the sensation of shearing tissue and eventually repositioning muscles in relation to something else, but what else? We did not know at that point. The ‘surgical’ and ‘muscle repositioning’ concepts seemed sound, but they didn’t explain the quality of firmness felt under the practitioner’s hands. We considered various concepts to describe this relationship. At some point, we noticed that the firmness under the hands arose when the touch related to the client’s wholebody weight.
Palpating a relaxed body on your table, it is difficult to sense its whole weight as the segments are free to move in relation to each other; in other words, there is slack in the system. Just as holding a piece of meat on a cutting board stabilizes it and helps with cutting, in fascial manipulation, firmness in the client’s body seem to optimize its effects.
Our finding is that combining a shearing with pressure, delivered in specific ways, engages the three-dimensionality of the client´s body, linking or integrating body segments so as to unify them in a single unit. Thus, the manual input evokes tensegrity in the system. Tensegrity evoked by touch can be seen (see Video1, listed in Video References at the end of the article) and also palpated when small sonar-like oscillations are imparted to the client’s body under the condition of fascial loading. With this shearing loading, body segments move in phase and in the same direction throughout the body. With ordinary oscillations (a slack system), the movement begins where the body first receives input and moves in waves in various directions through segments sequentially (see Figure 1).
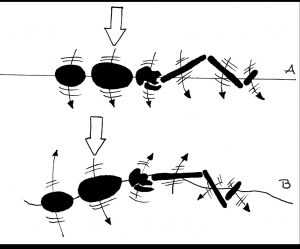
Figure 1: The effect of sonar-like oscillations under fascial loading (tensegrity) and under fascial slack. The white arrows show the vector of sonarlike oscillations manually imparted to the thorax. In (A), with previous manual loading of fascial system, the segments are integrated and move synchronously (in phase) in the same direction. In (B), without previous loading (slack system), segments are not integrated and move out of phase, in various directions. See also Video1. Illustration by Angela Lobo.
With tensegrity evoked, the practitioner can sense the client’s whole body weight (its center of gravity) as the segmental centers of gravity are linked. This provides the sense of a firm and steady platform that gives a counter-force to the practitioner’s input, and we assume this improves the ‘blunt-dissection’ effect. The key to evoking tensegrity is the way shearing and pressure are combined. Shearing alone drags tissues from superficial to deeper structures and at some point moves the latter in the direction of the shearing. Pressure alone squeezes tissues and dissipates the forces randomly. When shearing is combined with pressure with appropriate timing, quantity, and direction, it is possible to ‘corner’ deeper structures (especially bones) in relation to the previously loaded (sheared) tissue so that they are not dragged but rather stay still. There is thus a steady platform so that 1) tissues are not squeezed and 2) the force seemingly flows from the touch interface and concentrates wherever internal mobility among compartments is restricted. Adding minute torque, a third component of the touch, will ‘challenge’ the system and coax tissue differentiation (Figure 2). In this way, the shearing (bluntdissection) effects naturally occur where they are most needed, i.e., in areas with ECM densification and/or fibrosis, even in areas distant to the region of touch (Figure 3).
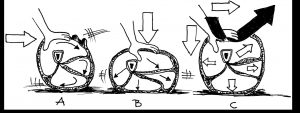
Figure 2: The combination of forces: (A) shear alone rolls compartments and drags bones along; (B) pressure alone squeezes tissues and forces are dissipated; (C) the appropriate combination of shear and pressure (white arrows) creates internal reaction forces that assemble the system and evoke a tensegrity response. Additional torque, represented by the black arrow, coaxes the differentiation of restricted tissue. Illustration by Angela Lobo.
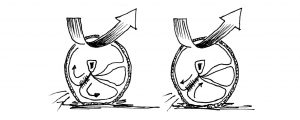
Figure 3: Two possible outcomes of differentiation between two myofascial compartments. With tensegrity, the interplay of internal forces between tension and compression elements may be such that shear vectors naturally concentrate/focus in areas of reduced mobility, which can differentiate (free) tissue restrictions even at a distance from the contact. Illustration by Angela Lobo.
It is our understanding that manually evoking tensegrity emulates the intercompartmental movements/relationships present in the client’s ordinary functioning. The firm platform created by tensegrity cause tissue restrictions to emerge in the direction of the practitioner’s hands, making palpatory diagnosis easier and more reliable, as such restrictions may have a functional significance.
Practitioner and Client Form a Single Tensegrity System
Further explorations showed that tensegrity in the therapist’s body favour its emergence in the client, i.e., ideally, client and the therapist form one single tensegrity system. Under such a condition, the practitioner can relate his own center of gravity to that of the client’s and, with proper positioning, rely mainly on his own weight to help free less mobile tissue (as opposed to the therapist adding muscle force), in a natural and effortless way (Figure 4).
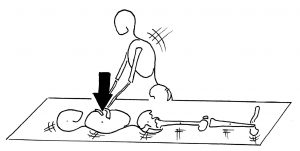
Figure 4: When practitioner and client form a single tensegrity system, any manual input will immediately transmit to the client’s whole body, providing a sense of firmness and security that favours therapeutic effects. Appropriate positioning also allows the therapist to use his own weight – as opposed to muscle force – to help free tissue. Illustration by Angela Lobo.
Curiously, the act of evoking tensegrity, ‘milking’ tissue from one hand to the other and loading the client’s system, seems to simultaneously load the practitioner’s system, evoking tensegrity in his own body. (We also use simple qi gong exercises to encourage self-awareness of tensegrity in the practitioner.) Unified in a single tensegrity system, both client and practitioner often subjectively recognize an appropriateness or ‘rightness’ to the condition (see the section on beneception below). We believe forms of bodily, nonverbal communication may be present, which will be subject of the second part of this article in a future issue.
Monitoring the Degree of Tensegrity
On starting a maneuver, it is common that not all the client’s body segments are integrated at once. For example, the thorax and pelvis may be integrated as a unit, but without the head. So, one can talk about degrees of tensegrity.
We use the oscillations described above to monitor the degree of tensegrity in the client’s body, observing which segments move in synchrony with the oscillations. Moreover, the small and precise oscillations allow both the practitioner and client to feel which segments are integrated at any given point of a maneuver. As the client can also feel the degree of tensegrity, this aspect of touch can be a resource to foster the client’s embodiment and also to strengthen the client-therapist relationship. Client’s and practitioner’s subjective experiences have also been shown to be useful in teaching this style of manipulation (Bertolucci 2010b)
It is also our observation that the degree of tensegrity tends to rise during the course of a maneuver, i.e., a progressively greater number of segments move in synchrony during the oscillations. We hypothesize that manually eliciting tensegrity evokes the spontaneous participation of the client’s system, leading to a progressively higher degree of tensegrity along a maneuver, as described below.
Spontaneous Motor Activity
At a certain point in clinical practice a curious phenomenon showed up: the practitioner sensing a push of the client’s head against his hands when working on the occiput. This action eventually became strong enough that the muscles’ action could be seen and palpated. Such observation led us to undertake EMG studies, where we detected an association between manually eliciting tensegrity and the arousal of spontaneous motor activity in the client’s body, namely, tonic activity of the spinal erectors. Working on either the occiput (Bertolucci 2008) or the thorax (Bertolucci 2010a), we detected tonic muscle activity in the cervical erectors.
The spontaneous motor activity took some time to start (around two minutes), progressively rose to a peak, then suddenly fell, at which time significant tissue release could be felt under the practitioner’s hands – and the client often referred to a relief or a release. To our knowledge, such a phenomenon has not been described in the literature before. Additionally, we detected synchronous cervical and lumbar erector activity, suggesting that the motor responses involve systemic mechanisms. We suppose that the progressive tonic activity underlies the (also progressive) degree of tensegrity observed during a maneuver, as mentioned above.
In some cases, the intensity of the motor responses became big enough to evoke involuntary movements, which sometimes continued even after manual contact ended (see Video 2). Indeed, we have already observed a myriad of motor patterns, such as twitches, clonic to-and-fro movements, slow undulating movements, and isometric co-contraction in yoga-like positions, among others. Slow eyeball movements were also observed, often in conjunction with altered consciousness (see Video 3).
The question naturally arose as to which physiological mechanisms were underlying those spontaneous responses. Taken together with another clinical observation described below, they suggest the involvement of autonomous homeostaticmaintenance functions.
Pandiculation: a Possible Link
A client complaining of neck pain had a first session. Returning for his next session, he mentioned the pain had gone. At some point he added, “I forgot to tell you that after our first session, I slept very well and the next morning, I deliciously stretched, which I have been doing every morning ever since. I then realized that at some point in my life I stopped doing the ‘morning stretch’, I don’t know why…” [Italics are ours, explanations below.]
The association to the patterns of involuntary movements we were already witnessing was obvious: they often very much resembled (and were experienced as) the behavior of pandiculation, the instinctive behavior of morning stretching and yawning. Would this client be ‘treating himself’ through resuming his habit of pandiculation? Curiously, the word he used in Portuguese was “espreguiçar” – a verb meaning ‘to take the laziness out’.
Pandiculation seems to be an appropriate model to understand the possible physiological mechanisms underlying the involuntary motor phenomena observed. Our current understanding is that there is a whole class of autoregulatory motor behaviors that work to restore and maintain the movement capabilities of animals. These could be considered akin to the morphogenetic movements seen in fetal development – in the sense that bodily movements are also determinants of morphology, given that they signal ECM modelling (and re-modelling) as discussed below. Pandiculation can be considered prototypical of such type of behavior. The effects would probably encompass both structural (e.g., myofascial) and neurological (e.g., tonic-postural function) effects (Bertolucci 2011).
Indeed, the phylogeny and ontogeny of pandiculation reveal its likely role in the development and maintenance of motor function. Fetal ultrasound studies on sheep (Fraser 1989a) revealed fetal pandiculation as a mechanism that influences functional determination of the moving parts of the musculoskeletal system and contributes to articular development and maintenance. Similar functions were also described in poultry, dogs, cats, and horses, among other animals (Fraser 1989a). In ostriches, a similar ‘maintenance’ pandiculation has been described (Sauer and Sauer 1967).
Pandiculation is described as a series of coordinated actions that unfold sequentially, building up soft-tissue contractile tension to a peak, at which point the joints of the limbs and trunk are maximally extended or, alternatively, the trunk is arched in flexion (Fraser 1989b). This is remarkably similar to the phenotype of the spontaneous motor activity we have been observing arising from Tensegrity Touch interventions.
Pandiculation-Like Reflexes?
It seems reasonable to postulate that manually-induced tensegrity stimulates receptors so as to create afferents that, once processed in various levels of the central nervous system (CNS), reflexly provoke involuntary pandiculation-like responses. Which receptors could be involved? As touch is mechanical stimulus, it is likely that mechanoreceptors are stimulated, especially interstitial receptors – rich in fascia – as well as the Ruffini corpuscles, related as they are to shearing forces (Schleip 2003); Pacinian corpuscles could also be stimulated during the oscillations. Receptors conveying interoceptive afferents (which monitor the physiological state of tissue, associated with maintenance of homeostasis) may also be involved. In fact, clients often experience interoceptive sensations during Tensegrity Touch maneuvers, such as dullness, burning pain, itching, changes in temperature. Such interoceptive sensations often have a hedonic value based on pleasantness or unpleasantness (Craig 2002; 2003) and may also work as a therapeutic resource in clinical practice, as mentioned below in the section on beneception.
I t i s a l s o wo r t h mn t i oig t hpossible involvement of non-neural, mechanoresponsive mechanisms such as morphological communication, in which morphology, physical forces, and displacements act as a non-neural channel of information (Rieffel et al, 2010), related as they are to tensegrity. This effect will be dealt with in Part 2 of this article in a future issue of this Journal.
Whatever the mechanisms involved, the involuntary tonic muscle activity of the pandiculation-like responses apparently aims – like the fascial manual input – to free structural restrictions (especially matrix densifications and fibrosis). This is what pandiculation itself seems to accomplish. This means that during a Tensegrity Touch maneuver the practitioner initially has an active role, blending manual forces so as to evoke tensegrity and, hence, the pandiculation-like reflexes. Those, in turn, progressively ‘take over’ the job of freeing such restrictions. In this sense, the practitioner works from outside in, while the client works from inside out – spontaneously – by means of the pandiculation-like reflexes. The clinical efficacy of Tensegrity Touch may be related to the summation of these effects.
Beneception, Nociception, and Homeostasis
A homeostatic behavior is any action that brings an animal back into homeostasis when an imbalance has occured. Interoceptive afferents inform the CNS so the required action can be planned and executed. The biological signaling in this process involves nociception and beneception (pain, pleasure, and related experiences).
For instance, when thirsty (nociception), the organism will search for water and be rewarded with pleasure (beneception) when drinking it (Esch and Stefano 2004). Similarly, it is uncomfortable to feel rigidity of movement and pleasurable when free movement is restored.
Interestingly, referred sensations triggered by Tensegrity Touch seem to convey some sort of biological meaning. We often hear from clients phrases like “ I feel parts being put in place”; “This touch is fixing such and such”; “This is the place where the problem is . . but it is not over yet; I feel some pain, but you can proceed because it is a good pain”; and so on. This kind of testimonial suggests that we have a system of recognizing the appropriate arrangement or relative positioning of parts/compartments within our bodies. Perhaps patterns of pandiculation arise from this interoceptive sensitivity? Indeed, interoceptive afferents have already been related to pandiculation behavior (Walusinsky 2006), as have temporary positional stress or immobility (Fraser 1989b) – that is, certains positions will create non-functional ECM links in certain areas that produce interoceptive afferents to the CNS, giving rise to the appropriate motor patterns to ‘free’ them. Maybe in Tensegrity Touch our way of evoking tensegrity somehow emulates the afferents that evoke pandiculation?
Tensegrity in Pandiculation and Somatic Disciplines
We now recognize tensegrity in virtually all life forms from micro to macro in scale. It is a way to build light, adaptable structures – and also possibly a way to help control movement other than through neural mechanisms, as noted above. Tensegrity is present in the evolutionary behavior of pandiculation, and also in classic somatic disciplines such as yoga and martial arts – where whole body actions and intersegmental relationships are acknowledged. Interestingly, some yoga poses are named after animal pandiculation behaviors, and martial arts movements also were often inspired by animal movements that exhibited tensegrity. Tensegrity and pandiculation are also found in more recent somatic modalities such as Eutonia, Continuum, Fascial Fitness, among others, each of which has its own way to encourage pandiculation and pandiculation-like movements.
Yawning and pandiculating in the presence of another person is considered rude in most cultures (Walusinsky et al. 2010). Do we have an embedded self-regulation resource (pandiculation) which education suppresses? If so, this may be one reason that musculoskeletal disorders are so common in our society.
Conclusion
ECM is under constant remodeling, reflecting our motor history. In this process, mechanical stimuli are determinant: good movement patterns reflect in healthy ECM and vice versa. For instance, normally gliding tissues tend to densify and adhere when there is no movement and/ or inflammation. This means that nonfunctional ECM molecular links are part of life, as there are periods of stillness (sleep), as well as vagaries like trauma and diseases that progressively diminish movement capabilities. Maybe pandiculation is a natural mechanism to re-regulate? Pandiculation patterns feature reaching to maximum body dimensions (Walusinsky 2006) – shapes of movement that seem to ‘refresh’ tensegrity through various body configurations. These intense stretching actions possibly free non-functional ECM bonds, restoring body architecture and at the same time stimulating tensegrity so that optimal movement patterns are perpetuated. Additionally, pandiculation resets postural muscle tonus to produce integrated movement, which in turn is a further source of good mechanical signals. In this sense, we could speculate that pandiculation is a form of neuromyofascial hygiene that is constantly restoring tensegrity.
If this is true, might we encourage pandiculation – and hence tensegrity re-sets – to enhance general health? This would require reassessment of cultural taboos against yawning and pandiculation, as well as further investigation of therapeutic approaches that could stimulate it. Tensegrity Touch seems to be one way to stimulate tensegrity and pandiculation through fascial touch in the Rolfing SI domain.
Part 2 of this article will describe additional Tensegrity Touch features as well as discuss their mechanisms of action.
Acknowledgements: Thanks to Angela Lobo, and Soraia Pacchioni for the theoretical and practical contributions, and to Anne Hoff for editing the text.
Luiz Fernando Bertolucci, MD, BSc is a biologist and physiatrist (rehabilitation medicine). He has been applying Rolfing SI in the treatment of musculoskeletal disorders since his certification in 1990. In this period he also developed Tensegrity Touch, and has been studying and researching its mechanisms of action. He is particularly interested in spontaneous selfhealing movements. He is on the Rolf Institute (RISI) Foundations of Rolfing SI Faculty and Fascial Anatomy Faculty. He teaches for the ABR (Brazilian Rolfing Association) and in health institutions in Brazil and abroad.
Angela Lobo has degrees in physical education and physiotherapy. She has been a Rolfer since 2004 and a part of the Tensegrity Touch Research Group since 2005. She is on the Foundations of Rolfing SI Faculty and teaches anatomy, physiology, and myofascial release for the ABR since 2009. She practices Rolfing SI and physiotherapy.
Bibliography
Bertolucci, L.F. 2008. “Muscle Repositioning: A new verifiable approach to neuromyofascial release?” Journal of Bodywork and Movement Therapies 12(3):213-224.
Bertolucci, L.F. and E.H. Kozasa 2010a. “Sustained Manual Loading of the Fascial System Can Evoke Tonic Reactions: Preliminary Results.” International Journal of Therapeutic Massage and Bodywork 3(1):12-14.
Bertolucci , L . F. 2 0 1 0 b . “ M u s c lRepositioning: Combining Subjective and Objective Feedbacks in the Teaching and Practice of a Reflex-Based Myofascial Release Technique.” International Journal of Therapeutic Massage and Bodywork 3(1):26-35.
Bertolucci, L.F. 2011. “Pandiculation: nature’s way of maintaining the functional integrity of the myofascial system?” Journal of Bodywork and Movement Therapies 15(3):268-280.
Chang, D.S., F. Burger, H.H. Bülthoff and S. de la Rosa S 2015. “The Perception of Cooperativeness Without Any Visual or Auditory Communication.” Iperception 6(6):2041669515619508.
Craig, A.D. 2002. “How do you feel? Interoception: the sense of the physiological condition of the body.” Nature Reviews Neuroscience 3(8):655-666.
Craig, A.D. 2003. “Interoception: the sense of the physiological condition of the body.” Current Opinion in Neurobiology 13(4):500- 505.
Esch, T and G.B. Stefano 2004. “The neurobiology of pleasure, reward processes, addiction and their health implications.” Neuroendocrinology Letters 25(4):235-251.
Fraser, A.F. 1989a. “Pandiculation: the comparative phenomenon of systematic stretching.” Applied Animal Behaviour Science 23(3):263-268.
Fraser, A.F. 1989b. “The phenomenon of pandiculation in the kinetic behaviour of the sheep fetus.” Applied Animal Behaviour Science 24(2):169-182.
Maas, H. and T.G. Sandercock 2010. “Force Transmission between Synergistic Skeletal Muscles through Connective Tissue Linkages.” Journal of Biomedicine and Biotechnology 2010(1):575672.
Sauer, E.G. and E.M. Sauer 1967. “Yawning and other maintenance activities in the South African Ostrich.” The Auk 84(4):571- 587.
Rieffel , J . A . , F. J . Valero – Cuevas , and H. Lipson 2010. “Morphological communication: exploiting coupled dynamics in a complex mechanical structure to achieve locomotion.” Journal of the Royal Society Interface 7(45):613–621.
Schleip, R. 2003. “Fascial plasticity – a new neurobiological explanation: Part 1.” Journal of Bodywork and Movement Therapies 7(1):11-19.
Walusinski, O. 2006. “Yawning: unsuspected avenue for a better understanding of arousal and interoception.” Medical Hypotheses 67(1):6-14.
Walusinski, O., R. Meenakshisundaram, P. Thirumalaikolundusubramanian, S. Diwakar, and G.
Dhanalakshmi 2010. “Yawning: Comparative Study of Knowledge and Beliefs, Popular and Medical.” The Mystery of Yawning in Physiology and Disease. Available at www.baillement.com/recherche/beliefs_ knowledge.pdf.
Video References
Video 1: http://tinyurl.com/ tensegritytouch1
Video 2: http://tinyurl.com/ tensegritytouch2
Video 3: http://tinyurl.com/ tensegritytouch3
Additional videos and articles are at the blog http://musclerepositioning.blogspot.com.br.Manually-Evoked Tensegrity and Pandiculation, Part 1[:it]Manually-Evoked Tensegrity and Pandiculation, Part 1