By Lina Amy Hack, Certified Advanced Rolfer™

ABSTRACT Mild traumatic brain injury (mTBI) is far from mild. In this article, Lina Amy Hack discusses one of her concussion stories as an example of the classic fall backward. The anatomy of coup and contrecoup brain injury is described and the resulting diffuse axonal injury (DAI) is explained. It is proposed that cranial nerves could be made more prominent in concussion research as it was Hack’s personal experience that her cranial nerves were directly damaged during the described injury.
Concussions are serious. When I first started reading concussion research, I took exception to the word ‘mild’ in the term ‘mild traumatic brain injury’, since all my concussions have felt really significant. So, I took a look at the definition of ‘severe brain injury’ which includes brain bleeds, broken skull bones, severed white tracts, and the list gets worse from there. Mild is clearly the low end of a progression that ranges to severe and life-threatening. In research, concussions are often called mild traumatic brain injuries (mTBI); they are closed head injuries (no skull fractures, no leaking fluids).
Concussions are difficult to diagnose because the damage is at the cellular level of the neural tissue and the symptoms are diffuse. They develop slowly over time in the acute phase of the injury (Ryan and Warden 2003). Since becoming a Rolfer I studied mTBI in part to understand my body’s story and also to be skillful for clients who present with this type of injury. In this article I will describe the anatomy of a common type of concussion that I happened to experience and the lesser- known injuries that follow.
When Rolfers do manual interventions with the heads of clients, they are interacting with all the mild head injuries the person has had. This article will increase your knowledge about the forces involved in mTBI, the tissue damage characteristic of concussions, and encourage you to pay attention to cranial nerves when working with the related biomechanics of a head that has a history of trauma.
Concussions are caused by either a direct blow to the head, face, or neck, or an indirect injury to the body that transmits force to the head (Hirad et al. 2019). The event could take the head from a stationary position and put it into motion; or the head could have already been in motion and the event could cause a sudden stop. The unifying idea is that the head undergoes a rapid acceleration and/or a rapid deceleration. Concussions were once thought to be negligible injuries (Ryan and Warden 2003). We now have substantial evidence that significant neurological changes occur: mTBI symptoms include cognitive injury (memory difficulties, decreased concentration, and decreased processing speed), somatic injury (headache, dizziness, nausea, fatigue, sleep disturbances, blurred vision, tinnitus, and hypersensitivity to light or noise), and affective symptoms (irritability, depression, and anxiety; Maruta et al. 2010).
Traditional treatment for concussions has been to rest until the symptoms have

abated. Now we have questionnaires to grade the severity of a blow to the head, and treatment includes giving the person information about post- concussion symptoms, what to expect during recovery, as well as possible light exercise regimes (McCrory et al. 2018). We now know that the pathology of a mild brain injury is due to axonal shearing of white tracts associated with the brainstem, corpus callosum, cerebral hemispheres, and cerebellum which interferes with normal brain functioning (Johnson, Steward, and Smith 2013). We could and should add cranial nerves to this list of structures that suffer axonal injury during mTBI. I like to think of cranial nerves as downstream tentacles from the upstream jellyfish brain, and when the latter gets bounced around the calvarium, the former experiences cellular changes.
Every concussion story is unique; an infinite number of trajectories of forces can connect with the head. As clinicians who hear clients’ mTBI stories, we have to deduce the individual mechanical experience of their head injury in order to strategize optimal manual interaction with the tissue. I present here my most recent concussion in 2004 as an example of a classic fall backwards. This type of injury is often explained in the mTBI literature, yet I invite you to think of this as the model to be applied to each unique circumstance you encounter. Another reason my example becomes useful to analyze is that it was a sports related injury, and a lot of concussion research is being done in the sports context. The sport I was playing at the time is called ringette (see Figure 1), which is an ice- skating sport that looks a lot like hockey but uses a straight stick (no blade) and a blue rubber ring (no puck). The players try to keep possession of the ring and score it into the net, which is exactly the same as a hockey net. Everyone is wearing helmets. In 2004 I was an upper- level ranking referee for ringette. I was refereeing a competitive playoff game for the age group of eighteen to twenty- year-old players; this was fast paced game. I was standing by the net, where the referee position is stationary, when a player with possession of the ring went behind the net with two attacking players on either side. The fast-moving group traveled behind my back; my eyes were tracking them first over my left shoulder. With a quick head pivot, I was expecting to catch sight of them again over my right shoulder. That didn’t happen. What did happen was they crashed into the back of me, took my legs out from under me, and my helmet-wearing head hit the ice- covered cement before the rest of me did.
There was an immediate shift of consciousness that I was not aware of at the time, I know now that I could not perceive that I was hurt as badly as I was. My training as a referee had me override my injury and push through. The play had continued down to the other end of the rink; no concern came my way, I popped up, caught up, and finished the game. The next morning when I woke up, my eyes were crossed; they didn’t uncross for an excruciating long time. A headache and confusion developed, worsening each day. I had trouble sleeping, I was nauseous, and six days after the event I saw a doctor who diagnosed a concussion. I was given information about symptoms that I would experience in the days ahead. The guidance was to not worry as concussion symptoms can get even worse before they get better. I had one month of memory loss after that. I learned to not be in distress that each day as I woke up, I couldn’t remember what I had done the day before. After about five weeks of feeling dizzy, sleeping a lot, and not being able to remember day-to-day events, these symptoms lessened.
Now, let’s deduce the intracranial forces involved in producing these symptoms. This is the common fall backward, where legs slip forward and the person’s occiput hits the ground. In this case the surface of the head had a helmet protecting it from contusions. Ideally, pre-fall, the person’s skull is functioning as the upper-most pole of the human structure, balanced on top of the spine (Rolf 1977), with a homeostasis to the pressure inside the cranial bones and the membranes and fluids secure in the skull.
We can think of the contents of the calvarium as the center of the central nervous system (CNS), home to thoughts. The CNS is the top of the body’s physiological regulation, and downstream from the CNS are vital senses like smell, sight, hearing, taste, and the vestibular system. The brain consists of highly organized neural cells and glial cells packed tight together and, interestingly, it has the consistency of jelly. The brain is wet in nature and is literally floating in cerebrospinal fluid (CSF), as CSF is 4% more dense than the brain (Drew and Drew 2004). Think of an enclosed buoyant jellyfish when imagining the brain (see Figure 2). Emerging from the
inferior aspect is the thick spinal cord also bathed in CSF, as it becomes part of the spine and looking a lot like the central thick tentacle of the jellyfish. Our jellyfish-like brain has small, fine tentacles as well; the twelve paired cranial nerves are tentacle-like fibers that originate in their respective nuclei of the deep brain (midbrain and brainstem). The cranial nerves have bundled axons that we call nerve fibers; the path of the cranial nerves involves tunnels into the various cranial base bones – they travel through to their respective sensorial or motor destination. The cranial nerves are wet in nature similar to the jellyfish-like tissue they came from. As they leave the skull, they are anchored via dura membrane and vascular fascia to the foramina they travel through (Barral and Croibier 2013).
Cranial nerves are rarely mentioned in concussion research, yet when I palpate the terminal structures of my cranial nerves on my own head, it feels as if I can access and work with my head injuries (Barral and Croibier 2013). Making contact with my frontal bone was the beginning of feeling the memory of that eye-crossing event, and providing gentle traction in an anterior direction gave me relief. It was contacting my sphenoid peripherally at the greater wings that I had access to the scar tissue that seemed concentrated asymmetrically behind my eyes. The best I can describe the feeling is a density that seemed to benefit from manually supported craniosacral motion of my sphenoid (Upledger and Vredevoogd 1983).
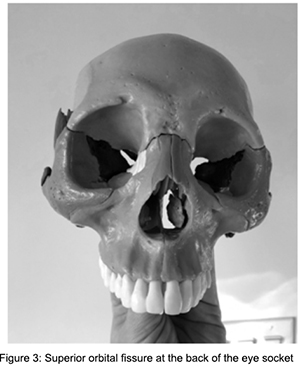
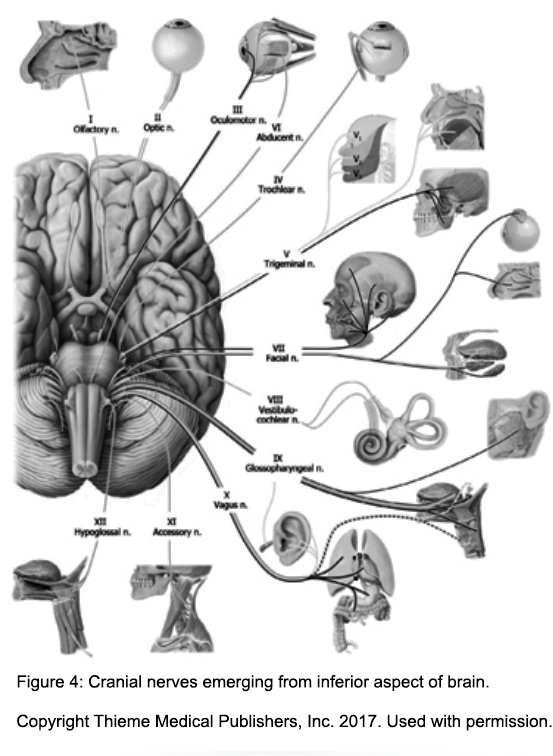
When I thought about the anatomy of my concussion that I was accessing, it felt less like compression in the sutures and more like something behind the eyes. Four cranial nerve pairs travel from their respective midbrain nuclei through the superior orbital fissure at the back of the eyes (see Figure 3): the oculomotor nerve (CN III), the trochlear nerve (CN IV), the abducent nerve (CN VI), and the ophthalmic branch of the trigeminal nerve (V1, see Figure 4). The first three of these innervate muscles that control eyeball movement. I mention the paired superior orbital fissures as an example to think broadly of all cranial nerves and all their foramina, for concussions can give all of the cranial nerves a stretch, which we will discuss in a moment. First, I want to mention another important passageway, the jugular foramina because they are the openings for the glossopharyngeal nerve (CN IX), the vagus nerve (CN X), and the
accessory nerve (CN XI) to travel through, as well as blood drainage for the inferior petrosal sinus and sigmoid sinus (see Figure 5). An mTBI could give an internal pull to these nerves affecting part of the functions involved in the muscles of the pharynx and larynx, the parasympathetic regulation of abdominal organs, and primary movements of the head. Some of the cranial nerves carry sensory information that travels from the periphery of the head to the CNS; some carry motor information that travels from the CNS to the destination; and some carry both. Regardless, all the functions innervated by the cranial nerves are essential and are directly involved in survival. At the cellular level, these tentacle-like fibers are really collections of tens of thousands of axons of nerve cells emanating from the midbrain and brainstem.
Now we’ve got our working model of the head, we can return to the example mTBI of the standing person about to fall. Imagine in slow motion the skull with the floating jellyfish-like brain falling backward, and the helmet-covered head hitting the ground. What happened in those quick moments is essential to understanding the injury. As the skull is falling, the forces in the tissues vary because tissue densities vary: dense bone is falling, the CSF is falling, the enclosed jellyfish-like brain is falling, and the cranial nerves are falling. The skull bones are stopped first by the ground with a rapid deceleration. The location that is struck is called the ‘coup’, in this case the occipital region.
This is where the person may experience a contusion, bruise, and pain. A contusion did not occur in our example as I was wearing a helmet. But there was an injury: concussions are an injury inside the calvarium. Once the bone stops, the fluid experiences a rapid deceleration. One might suppose that it slops around, but in actuality the fluid is quite contained and it is quickly subjected to the mass of the brain smashing into it. The brain pushes into the CSF and then the inside of the bone – this is the internal coup. And there is a second location of injury in the skull in that moment, exactly on the opposite- side skull interior; this is the ‘contrecoup’. The forces involved at the contrecoup are more severe than at the coup, and the brain injury tends to be more serious at the contrecoup (Ramzanpour et al. 2018).
There are several theories about why the contrecoup brain injury location incurs more damage than the coup:

for tissue to travel in a linear way when experiencing sports-related forces, there is often a rotational force experienced by the skull and brain as well (Drew and Drew 2004). The falling jellyfish-like brain in our example is suddenly stopped and the contrecoup location is subject to a combination of linear movement as well as rotational movement, which can induce shear rotational forces through the midbrain and brainstem cranial nerve tracts with an unfortunate focal point of stress at the contrecoup location.
Angular acceleration theory: In physics, the idea of an angular acceleration is that the object (here the brain) that is experiencing the sudden deceleration is tethered to an object of dense mass (here the skull), where the first object will change speed more slowly than the mass it is tethered to and will experience angular forces through the tension of the tether itself (Drew and Drew 2004). The brain is mostly a free-floating jellyfish-like object, as we have already discussed, yet it does have anchors and compartments.
The seven pairs of cranial nerves that emerge from the midbrain and brainstem (CN VI, VII, VIII, IX, X, XI, XII)
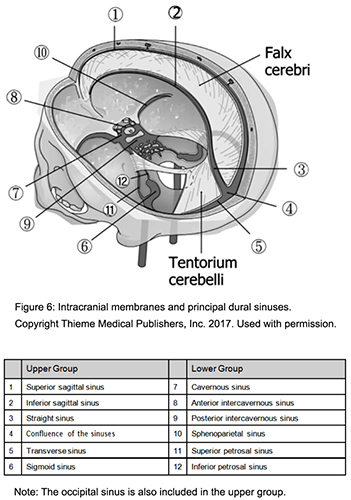
travel short distances before piercing the sphenoid, temporal, and occipital foramina, where their dura will merge with the fascia of the bone, becoming an anchor of sorts to a decelerating brain. Another anchor for the brain and CSF system occurs where the dura mater is continuous with all four clinoid processes of the superior sphenoid, as well as the connection between dura and the foramen magnum (Upledger and Vredevoogd 1983). The dura mater along the inside of the skull also folds inward to create internal walls: the falx cerebri, falx cerebelli, and the tentorium cerebelli (see Figure 6). Right where these membranes meet the skull there are vascular venous sinuses in the fold of the dura against the skull; the blood and fluid collecting here is about to flow out of the brain. The brain is not attached to these vascular and membranous structures, but the brain is subject to their shape and all concussion forces would take place inside these compartments.
In that split second when my legs went out from under me and the back of my head and body slammed to the ice surface, my brain experienced an injury from the mechanical forces converging at the contrecoup. Being so engrossed in my role as referee, I popped back up to my feet and got back to the game. I probably looked exactly the same to the spectators, players, and coaches, but what I know now is that in that split second on the ice, my brain had been cushioned on its posterior side by the helmet, by the skull, and by the accumulating CSF. The brain bounced. The negative pressure at the contrecoup would have put a stretch into the anchored cranial nerves, and rotational shear forces would have occurred between the midbrain and
brainstem, especially along the uneven surface of the superior sphenoid. Brain tissue that was tethered would have had angular stretch forces exerted through its cellular fibers; some tissue would have been suspended in CSF with different vectors of deceleration, creating the opportunity for multi-vector shear throughout the inferior aspect of the brain. This injury did not produce immediate impairment – no loss of consciousness, and no loss of motor function. Yet the cognitive, somatic, and affective symptoms that developed in the days that followed gave me direct knowledge of the respect this type of injury deserves.
The reason that mild head injuries have a slow onset of symptoms is that neural cells don’t die at the moment of the injury during an mTBI; the neural cells in the white tracts that get the shock wave maintain their cellular membrane integrity initially. The damage is inside the neural cell. Like we’ve covered, cranial neurons have a cell body, this is where the proteins are made, genetic code is stored, and mitochondria produce biochemical energy for the cell. Cranial neurons also have a long tube-like axon, which carries the neural signal either from the brain to the motor destination or from the sensorial periphery to the brain. For example, the cell body of a neuron belonging to the glossopharyngeal nerve (CN IX) can be found in the medulla part of the brainstem; its axon will emerge as part of the neuron, pass through a jugular foramen heading toward the pharynx, sending signals regarding swallowing. You can think of that axon as a microscopic tube of fluid. This tube of cytoplasm also has cytoskeleton filaments in it that travel the entire length of the axon, all the twists and turns. There are neurochemicals at the terminal end of the axon that need to be transported all the way to the cell body in the brainstem and vice versa. There are neural peptides made in the cell body of cranial neurons that need to be transported from the brainstem, down the axon tube, to the terminal button. There are many of these microtubules in each axon. These cellular fibers maintain the shape of the neural pathway as it has corners through the bone and microtubules also serve as scaffolding for these transporting proteins. They are like stationary elevator cables where transport proteins will pull along the cytoskeleton to move important cellular molecules. It is these microtubules that break during an mTBI causing the axons to lose their shape; this damage is called a diffuse axonal injury (DAI). The symptoms that a person experiences after this kind of injury emerge slowly over time: delayed-onset of headache, dizziness, and confusion are now recognized as post- concussion symptoms due to DAI (Ryan and Warden 2003).
Putting it all together, concussions occur when neural cells in the skull and their axons experience mechanical stretch, shear, and rotational strains at the moment of rapid acceleration/deceleration leading to the axons becoming stressed, undulated, and misaligned as a result of axonal cytoskeleton damage. DAI is difficult to diagnose because in vivo imaging of this microscopic breakage is not available. From personal experience, I could feel the change in my head’s cellular environment yet I could not have described it. Once microtubules are broken, transport molecules that were moving along start to accumulate at the breakage points. This happens slowly in the hours after the event. There is a range of severity to axonal swelling depending on the forces each axon experienced. At first the breaking of the microtubules may allow relaxation of the tension in the axons, but the cell suffers interrupted axonal transport and ballooning of cytoplasmic fluid. A neuron with a low-grade axonal injury will still be able to conduct its neural signal and it may be able to be repaired; it is still a living cell. Cellular molecular machinery may be able to rebuild and reconnect the microtubules. The fluid involved in the swelling may be moved along the remaining intact microtubules. Flow can be restored to both the internal molecules and the action potential signal along the axon membrane
– this takes time. The damaged axon may experience partial interruption of axonal transport from staggered breakage points among the microtubules; these axons may swell along their entire length and still function well enough to send neural signals but in a compromised state. A concussed brain has altered neural signal speeds due to DAI; the body of the neural cells living in the brainstem experiences changes in its mitochondria, which decreases the energy reserves of the injured neurons. Sometimes
this compromised quality of neural signal can become a persistent dysfunction (Johnson, Steward, Smith 2013).
The day after my concussion while refereeing I woke up with my crossed eyes, they wouldn’t uncross for what felt like a long time. I had no idea what was going on nor how serious a symptom this was. Fair to say the swelling in my cranial nerve tracts had been progressing while I had been sleeping: mTBI research has found that axonal pathology increases to a peak in the first twenty-four hours following the head trauma and levels off after that (Johnson, Stewart, Smith 2013). Significant axonal swelling can get critical and look like a bulb along the axon, even if it doesn’t burst the cell; a large axonal bubble will essentially cause a disconnection to the axon’s ability to function. Disconnected axons become broken cell junk that the cellular community in the brain has to clean up – this takes time. Glial cells and immune cells will break down the material of the axon and over time, absorb the components or allow the degraded axon parts to flow downstream interstitially into the lymph system of the brain, which flows to the aforementioned sinuses (Yao et al. 2020). The loss of axons is eventually visible and measurable as shrinking white tract structures in the brain. Hirad and colleagues (2019) found there was a reduction of thickness of white brain matter in the right midbrain structures of collegiate football players at their postseason assessment compared to their preseason assessment. Players that had more mTBI events with rotational acceleration features had the most loss of white matter, including structures associated with the brainstem. They also found a significant correlation between decreased white brain matter and neurocognitive changes with the athletes.
In our example, now that we have all the pieces, we see that my helmet protected the surface of my head so I was able to pop up and keep going. Yet due to the snap of head hitting the ice, my jellyfish-like brain with cranial nerve tentacles experienced a quick deceleration with rotational and angular forces. The convergence of shock led to a significant contrecoup injury; my brainstem and deep brain structures were likely pulled away from their cranial base foramina, yanking on my cranial nerves as they travelled their winding routes through bone, shearing microtubules in cranial neurons. It is my thought that both sides of my oculomotor nerve (CN III), trochlear nerve (CN IV), and abducent nerve (CN VI) that together travel through the superior orbital fissures of the sphenoid had such an abrupt tensioning that there was significant DAI along those motor fibers. This led to peak axonal swelling the next morning and the muscles of my eyes were on the receiving end of failing neural signals; since my cranial nerves were delivering faulty signals, my eye muscles could not straighten my eyeballs.
Healing from a concussion takes time; the first step is realizing that the concussion has happened. In the moment that I had no control over the direction of my eyes, headache, dizziness, and confusion were prominent; still I was not aware that I had an mTBI. Asking the brain to perceive its own injury is dubious. I remember willing my eyes to bring their focal points back together, resting them closed when they couldn’t, then trying again. When my eyes did return to me, they stayed with me; they clicked ‘on’ again. With the neural activation of attention along those cranial nerves, I showered those pathways with signals to animate my eyes properly. Eventually, the signal found a way around the swelling axons to an intact circuit. This is what neural plasticity is all about: when a familiar pathway becomes damaged, the brain can adapt to use an intact axon on an neighboring route to deliver the message, producing a new circuit along the same nerve, and leading to functionality again (Doidge 2007).
In the days following an mTBI, the damaged cell structures associated with the bulbous axons become broken down producing interstitial junk. The brain has its own lymphatic system called the glymphatic system. This is a network of lymph vessels that receive the downstream interstitial fluid and the waste products from the neurons and glial cells (Yao et al. 2020). This is how the brain removes broken down materials that are too large to diffuse into the blood stream on their own; glymph
appears to be a unique lymph as it is also downstream of CSF biomolecules. It has been proposed that manual therapy of the head after concussions supports the flow of the glymphatic system (Yao et al. 2020) as well as CSF movement associated with the cranial bones (Upledger and Vredevoogd 1983).
In my concussion example, I had a second reason to be in denial about my injury: it happened five days before my wedding! By the time of my wedding, it was clear to me and my loved ones that I was suffering the symptoms of a concussion. I could only think one thought at a time. I remember as I watched my friends and family pack up all my stuff the day after the wedding, that I was not capable of the complex thinking involved in packing up. It took a lot of effort to plan out how I was going to get out of the chair I was sitting in and to focus on getting across the room. If I thought about the future or the past, my head pain would increase. My own body taught me how to heal from this injury; it had me slow right down. I had to let go of things like remembering day to day events, to rest without any stressful demands to my performance; it was many days with very simple thinking (see Figure 7). After about a month, almost like a light switch, I could feel my capabilities come back to me; luckily new neural circuits were ready to go for me.
In this discussion we stayed on the mild side of the concussion symptoms in that we side-stepped discussing loss of consciousness due to a blow to the head – some people go into a coma after an mTBI. We also stayed focused on brainstem structures, while it is also true that all the brain structures suffer the forces of mTBI. I focused on the brainstem/cranial nerve connection to illustrate my specific symptoms. There is a wide range of individual differences between concussions. For brevity, I also skirted around downstream consequences such as brain swelling associated with head injuries and oxidative stress that increases after mTBI. There is sometimes inflammation in the meninges and brain parenchyma which can co-occur with DAI (Yao et al. 2020). The myelin sheath around axons is protective to concussive forces, yet there is a complex nuance there that was beyond this discussion.
I invite you, the reader, to take a pause, close your eyes, and feel the space behind your eyes – does it feel level with the horizon? Invite your hands to your temples to give touch feedback about the horizon behind the eyes and follow the micromovements from there, you may find your own mild injuries ready to surface and be soothed.
Lastly, the next time you hear a client talk about a concussion, I invite you to imagine the forces of acceleration and deceleration that were unique to their experience, to deduce where the coup and contrecoup occurred. As we have reviewed, concussions are serious.
Lina Amy Hack has been a Rolfer since 2004, practicing in Saskatoon, Saskatchewan, Canada. She came to Rolfing SI as a biochemist who had done genetic engineering research after her honours BSc, later working in a water quality testing. Since becoming a Rolfer she has become a Somatic Experiencing® Practitioner, completed a BA psychology honors undergraduate degree, researching parental touch patterns and child sleep behavior. She completed her Advanced Rolfing Training in 2016. Lina is also the Co- Editor-in-Chief of this journal.
Banga, M.S., BV, S., Roy, K., Saha, S.K.,
Dixit, S., and P. Ghosh. 2017. Contrecoup head injury. Indian J Neurosurg, 6:103-106.
Barral, J-P. and A. Croibier. 2013. Manual therapy for the cranial nerves. Palm Beach Gardens, Florida, USA: Barral productions.
Doidge, N. 2007. The brain that changes itself: Stories of personal triumph from the frontiers of brain science. New York: Viking.
Drew, L.B. and W.E. Drew. 2004. The contrecoup-coup phenomenon: A new understanding of the mechanism of closed head injury. Neurocritical Care, 3:385-390.
Johnson, V.E., W. Stewart, and D.H. Smith. 2013. Axonal pathology in traumatic brain injury. Experimental Neurology, 246:35-43.
Hirad, A.A., J.J. Bazarian, K. Merchant- Borna, F.E. Garcea, S. Heilbronner, D. Paul, E. B. Hintz, E. van Wijngaarden, G. Schifitoo, D. W. Wright, T.R. Espinoza, and B.Z. Mahon. 2019. A common neural signature of brain injury in concussion and subconcussion. Science Advances, 5(8):1–11. https://advances.sciencemag. org/content/5/8/eaau3460 (accessed December 9, 2020).
Maruta, J., S.W. Lee, E.F. Jacobs, and Ghajar. 2010. A unified science of concussion. Ann NY Acad Sci 1208:58–66.
McCrory, P., W. Meeuwisse, J. Dvorak, M. Aubry, J. Bailes, S. Broglio, R.C. Cantu et al. 2018. Consensus statement on concussion in sport—the 5th international conference on concussion in sport held in Berlin, October 2016. Br J Sports Med, 51:838:847.
Ramzanpour, M., A. Eslaminejad, M.Z. Farid, M. Ziejewski, and G. Karami. April 2018. Comparative study of coup and contrecoup brain injury in impact induced TBI. Biomedical Sciences Instrumentation, 54(1):76-82.
Rolf, I.P. 1977. Rolfing: The Integration of Human Structures. New York: Harper & Row.
Ryan, L.M. and D.L. Warden. 2003. Post concussion syndrome. International Review of Psychiatry, 15 (4): 310-316.
Upledger, J.E. and J.D. Vredevoogd. 1983. Craniosacral Therapy. Seattle, WA: Eastland Press.
Yao, S.C., H. Zwibel, N. Angelo, A. Leder, and J. Mancini. 2020. Effectiveness of osteopathic manipulative medicine vs concussion education in treating student athletes with acute concussion symptoms. The Journal of the American Osteopathic Association, 120(9):607-614.