
In this article I want to facilitate an enhanced awareness of major physiological conditions the body goes through that highly influence the internal and external organisation of pelvic structure and psoas function. Some of the bony and functional dysfunctions are protective patterns associated with organs ranging from kidneys to the ovaries and the prostate. These patterns allow for better organ function. If eliminated without first helping the inner tissues, this will cause an inflammatory episode of a chronic inflammation or malfunction of the organ. If treated with respect and care for all tissues, we can help the body to come to a higher level of reorganisation and recuperation of its own healing properties.
The Case of Inflammation
Inflammation can be caused by microbes (such as bacteria, virus, fungus, etc), physical trauma, and overuse of tissue. All of us have undergone intestinal inflammations; many of us have had infections of the bladder, kidney, ovary, spermatic duct, prostate, and others that directly influence the organization of the pelvic ligaments and musculature crossing the pelvis and thus the spatial arrangement of the pelvic bones. Many of us have gone through inflammatory processes caused by physical trauma of various origins.
All of these inflammations have typical stages with typical physical reactions to them:
There are different courses an inflammation can take:
Acute: the inflammation goes through all typical stages and heals mostly completely (restitutio ad integrum).
Subacute: the presence of an inflammation does not become as clear, the bodily responses are often not strong enough to completely heal, persistent defects occur.
Chronic: not complet ely healing, reoccurring episodes, persistent defects may get stronger with each episode.
Subsequent: other tissues get overused by trying to bridge joints that are lacking normal motion and function of tissues in a functio laesa-state or after necrosis.
Typical persistent defects are, among others: ongoing chronic inflammations, with swelling, heat, pain; and adhesions in the surrounding tissues, which cause irritation and pain. These irritations trigger uncoordinated muscular activity, fascial strain patterns, and exaggerated muscular responses, or there can also be a remaining protective pattern of avoiding any tonus of the surrounding musculature and fascia in order to inhibit further responses of the organs, muscles, and tissue and in residual scars.
It seems to me that many imbalances in the body are caused by remaining patterns of functio laesa, where body and often psyche are stuck in the stage of an inflammation or trauma reaction and have somehow not come to the full end of the healing cycle. Thus body and soul have not come to the realization of the fact that it is over.
If we have a look at the effects on the surrounding tissues, we find that inflammations have a tendency to travel along certain routes. Different bodies seem to have different preferences. For some it will mostly be the lymphatic travel-paths, including interstitial liquids; for some, the nerves or blood vessels; for some, the ligaments, and for others the muscular fascia.
Glands normally will have a lymphatic activation, but the prostate, for example, often causes direct co-inflammations of the ligaments from sacrum to prostate/urethra (the male equivalent to the sacrouterine ligaments). Inflammations of the intestines or tubes / ovaries, spermatic ducts / prostate, and even bladder have a tendency to be stronger on one side of the body than the other. The inflammation will first cause an activation and shortening of the ligament. Thus a co-inflammation of these ligaments will cause an inner pull on the sacroiliac joint that leads to a block of movement there. The sacrum will deviate from its normal position, and all muscles of the area will have to form stabilization chains to counterbalance. Due to the inner swelling of the tissue in the whole area and the increased circulation, there will be a dull pain in the lower back. Figure 1 shows the uterine ligaments.
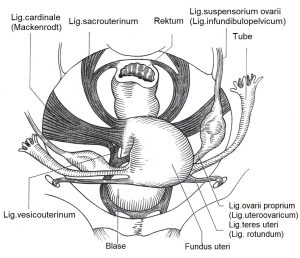
Figure 1: Uterine ligaments (from Martius Hebammenlehrbuch, Thieme-Verlag, 1984).
With a chronic inflammation the body can come to the other extreme of reaction: repressing all nerve information coming from an area and deactivating the local ligaments and structures to stop the constant alarm. A reactivation through Rolfing® Structural Integration and Rolf Movement® work thus might reawaken an old pain or cause an episode of a chronic infection. Both have to be seen as opportunities for healing. In case of the chronic infection, the body might finally have the power to heal, or the person can see a health practitioner who treats the disease. Reorganizing the area through fourth-, fifth-, and sixth-session work from the Rolfing Ten Series might help bring the organ to a spatially more healthy position, where the body’s own properties of healing can work better.
With kidney infections, or trauma in the back at the level of the kidneys, we often have an influence on the psoas (see Figure 2). It can either be stuck in hyperor hypotonus. It can also be completely deactivated, generally on one side more than the other. Delicately applied psoas work can considerably help a kidney that is in trouble. As we all know, when a psoas is not active, the iliacus will try to help the situation; thus, depending on which portion of the iliacus is more active, the ilium might get pulled into anterior tilt or the hip joint might get fixated. This will influence the position of the sacrum and influence all other ligamentous and muscular balances of the pelvis.
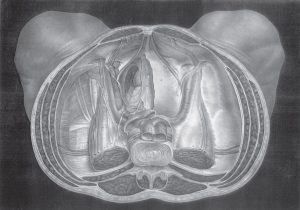
Figure 2: Inside the pelvis (from Iconografia d’Anatomia Chirurgicadi Medicina Operatoria, by Dr. J. M. Bourgery, Serantoni Editors, Florence 1856, courtesy of Pierpaola Volpones).
The Influence of Pregnancy
Another example I want to roughly sketch out is changes due to pregnancy. Ligamentous stretch through the influence of the hormones starts right at the beginning of the pregnancy. Muscular stabilization has to take over. Some women create stabilization in upright position more through muscular action, while others lean into their ligaments a lot. For the latter, already in early pregnancy, this represents a big shift in the method used to stabilize the body. They have to relearn stabilization, and will have a tendency to sacroiliac joint problems early in pregnancy, when the increasing weight cannot yet play a sufficiently explicative role. The pubic symphysis can increase its physiological deviation from a few milimeters to a whole inch (2-3 cm.) and in some cases up to 2 inches. This of course influences all surrounding tissues and is a major task for stabilization in motion.
In utero, most babies have a preferred position. If the baby’s back is on mother’s left side, the mother’s psoas on that side will have to react, because the head of the baby is being pushed towards the ilium more often and more strongly than on the other side. At first that muscle might react with contraction, but over the course of time it will become more deactivated. According to gynaecological literature, 60% of babies prefer their back to be on mother’s left side.1 The push of the baby’s head will often cause the ilium to come into anterior tilt: the ligaments of the sacrum, and the organization around the sacrum (including the piriformis), will try to counterbalance. Many times these patterns will persist after delivery. Rolfing work can help a lot to support the client coming back into balance.
Conclusion
Knowing our clients’ histories will help us to make an informed assessment of where to work and what to expect as probable reactions to our work. It will also help us prepare our client’s awareness for physiological healing reactions.
Endnotes
References
Barral, J.-P. and Pierre Mercier, Visceral Manipulation. Seattle, WA: Eastland Press, 1998.
Barral, J.-P., Viscerale Osteopathie in der Gynaecologie.Munich: Urban & Fischer, 2004.
Calais-Germain, Blandine, Le perinee feminine. Micropolis: Edition Desiris, 2000.
Carrier, Beate, Beckenboden. Stuttgart: Thieme, 2003.
Hees, Sinowatz, Allgemeine und Spezielle Pathologie. Cologne: Deutscher Ärzte-Verlag, 1996.
Martius, Hebammenlehrbuch. Stuttgart: Thieme-Verlag, 1984.
Meert, Guido, Das Becken aus osteopathischer Sicht. Munich: Urban & Fischer, 2003.
Pschyrembel and Dudenhausen, Praktische Geburtshilfe. Berlin, New York: de Gruyter, 1986.
Schultz, R. Louis, Out in the Open. Berkeley, CA: North Atlantic Books, 1999.
Tanzberger, Kuhn and Moebs, Der Beckenboden- Funktion, Anpassung und Therapie. Munich: Urban & Fischer, 2004.