
Whenever someone comes into my office with temporomandibular joint (TMJ) dysfunction, I can’t help but cringe a little. And when I hear practitioners crow about how they always have great luck “curing” TMJ, I cringe a little more, and reckon that either (a) they get really fresh, easy cases, (b) they are extremely lucky, (c) they have a corner on the magic, or (d) they are deluded. For the truth is that the TMJ is an extremely complex anatomical system, subject to many influences both within and outside of the context of Rolfing® Structural Integration, and that using other paradigms sometimes needs to be considered. From my perspective, cranial manipulation often fills the gaps that fascial work can’t, because the worst cases of TMJ dysfunction involve derangements of the articular disc, situations that call for more than straightforward tissue work.
Analyzing all the influences on the TMJ that could emanate from the cranial system would take volumes, well outside the scope of this piece. Simply, they could derive from forces acting upon the mandible, temporal bone, and the intracapsular disc from the other neighboring bones of the cranium, the dura and cranial membranes, and fascial chains extending down the body. Unless these forces are resolved, they can persist in holding the TMJ structures out of balance ad infinitum. If the cranial system is suspected as being a significant influence in the TMJ dysfunction, a referral to the appropriate practitioner may be advisable. For our purposes, we will limit ourselves to an overview of the immediate environment of the TMJ itself. There are several thorough articles dealing with TMJ myofascial influences written by our colleagues Clay Cox (2001), Christoph Sommer (2008), and Peter Schwind (1987), and I won’t repeat what they have already said; derangements of the articular disc are a separate entity and a primary cause for the worst cases of TMJ, issues of persistent jaw clicking and locking.
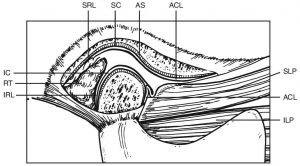
Figure 1: Temporomandibular Joint. Diagram showing the anatomical components: ACL – anterior capsular ligament (collagenous); AS – articular surface; IC – inferior joint cavity; ILP – inferior lateral pterygoid muscle; IRL – inferior retrodiscal lamina (cartilaginous); RT – retrodiscal tissues; SC – superior joint cavity; SLP – superior lateral pterygoid muscle; SRL – superior retrodiscal lamina (elastic). The discal (collateral) ligament has not been shown. All images used with permission.
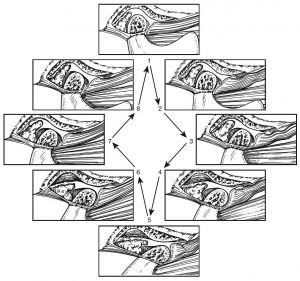
Figure 2: Normal functional movement of the condyle and disc during the full range of opening and closing. The disc is rotated posteriorly on the condyle as the condyle is translated out of the fossa. The closing movement is the exact opposite of opening. The disc is always maintained between the condyle and the fossa.
A good grasp of the biomechanics of the TMJ is important in having a clear picture of TMJ dysfunction. The most significant aspect is the balance of tensions on the disc. The articular disc is bound to the mandibular condyle with its head contacting the disc’s “intermediate zone,” and is sandwiched between the condyle and the articular surface of the temporal bone. This creates a cushioned, sliding contact for the two bones. While there is a degree of lateral/medial motion of the disc, its anterior/posterior freedom is our most significant concern. Posteriorly, the disc is attached to the retrodiscal ligaments, bungee-like structures that act to keep the disc in position, with its intermediate zone centered on the condyle. The ligament tensions are balanced anteriorly by the lateral pterygoid muscle (more specifically by its superior head), part of which is directly attached to the disc, with the rest of the muscle inserting on the mandibular condyle (see Figures 1 and 2).
While there is some controversy surrounding the details of disc and lateral pterygoid function, most sources agree that a hypertoned superior lateral pterygoid can lead to derangement of the disc. The muscle will exert an anterior pull, putting a strain on the disc and the superior retrodiscal ligament when in the resting position. With prolonged tensions, retrodiscal integrity can degrade and the disc will distort over time and will slip forward. The net result is a migration of the disc’s contact surface on the condyle from its intermediate zone more posteriorly, thereby altering the biomechanics. The degree to which the disc is affected will contribute to whether it develops a click, displaces and repositions (is reduced), or displaces without reduction

Figure 3: Functionally Displaced Disc. Tension on the disc has shifted its position posteriorly from the intermediate zone when at rest. (This is step 1 in the motion sequence of Figure 2; clicking occurs between steps 2 and 3, with a reciprocal click between steps 8 and 1 as the condyle slides between the different sections of the disc.

Figure 4: Anteriorly Dislocated Disc with Reduction. A: Resting closed-joint position (step 1 in Figure 2). B: During the early stages of translation, the condyle moves up onto the posterior border of the disc (reduction). This can be accompanied by a clicking sound (steps 3-4). C: During the remainder of opening, the condyle assumes a more normal position on the intermediate zone of the disc as the disc is rotating posteriorly on the condyle. During closure the exact opposite occurs. In the final closure the disc is again functionally dislocated anteromedially. Sometimes this is accompanied by a second (reciprocal) click.
Clicking in the joint is caused when the condyle shifts on the disc during its motion cycle. If the disc has migrated to the posterior zone for a period of time, it distorts and the disc body thins, allowing it to shift forward, forming a “cup” for the condyle to rest in. During opening, a single click will coincide with the shifting of the condyle over the lip of the cup, and sometimes a second click will occur when it slips back to the posterior zone (see Figure 3). A more serious condition will arise when the retrodiscal ligaments are further stretched, with the disc actually being dislocated forward off the condyle during rest. Upon opening, the disc may reduce (reposition), but dislocates again on closing. The sliding onto and off of the disc will create clicks as well (see Figure 4).
The worst cases are disc displacement without reduction, when the disc slides anteriorly, completely off the condyle, and does not reduce. In such a “closed lock” condition, the disc blocks the condyle from sliding forward. It is not literally locked, but its opening is severely limited on that side (see Figure 5). “Open lock” conditions are likewise serious, and typically occur as a “spontaneous dislocation,” when the condyle is forced open beyond its normal range. The condyle displaces off the disc and is stuck forward, beyond the articular eminence on the temporal bone. In an open lock, the disc can be located either in front of or behind the condyle and the jaw won’t unlock because it is mechanically blocked by the eminence. The disc and retrodiscal tissues can be crushed between the bony contacts and stretched or torn (see Figure 6).

Figure 5: Anteriorly Dislocated Disc Without Reduction. The disc becomes jammed forward in the joint, preventing the normal range of condylar translator movement throughout the entire sequence shown in Figure 2. This condition is referred to clinically as a “closed lock”
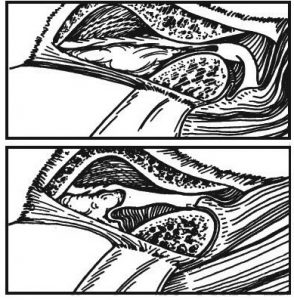
Figure 6: Spontaneous Dislocation of the TMJ. Spontaneous dislocation of the condyle at step 5 (in Figure 2) results in an “open lock” with the disc dislocated anterior or posterior to it. The condyle is trapped beyond the articular eminence.
Dislocation without reduction (closed-lock) conditions are liable to create damage that is irreversible over time, because the disc is trapped in front of the condyle and its associated support structures are deranged when the jaw is at rest. The longer the disc stays out of place, the worse the damage to the tissues. The retrodiscal tissues stay under tension and are stretched, and the disc itself gets further misshapen. It is best to reposition the disc with as little delay as possible. Gently gapping the binding there by gently pushing down on the chin or at the molars may un-jam the block.
Assessment is generally straightforward. Note the position of the mandible with the jaw closed. If it is off-center, one side is in open-lock, deflecting the mandible to the opposite side. If the mandible appears centered, have the client open his mouth. If there is deviation to one side and then recovery, there is dislocation with reduction on the side to which the mandible deviates; if there is no recovery, there is typically either no reduction, an adhesion of the disc to the temporal bone, or a muscular spasm on that side.
Prior to any attempt to reposition the condyle or disc, it is important to defuse the tensions on the TMJ as best as possible. From a Rolfing® Structural Integration perspective, this includes all fascial structures related to the mandible, including the hyoid musculature. The lateral pterygoid is primary because it provides the anterior force on the disc. It is then necessary to open the disc space in order to free the structures. Then, the condyle needs to be moved anteriorly in order to reposition itself on the disc.
Sometimes it is possible for the client to self-reduce the problem disc by opening slightly and sliding the mandible to the opposite side. This action translates the ipsilateral condyle anteriorly, engaging the superior retrodiscal ligament, and hopefully drawing the disc posteriorly into reduction. Several tries can be made before the practitioner attempts reduction. If unsuccessful, the practitioner can then try to reduce the disc.
To work with the TMJ, it is important to use a secure position that stabilizes the head and allows good motion at the joint itself. With one hand, hold the mandible with the thumb intraorally along the molars, the forefinger outside along the jawline toward the angle, and the other fingers wrappin around the jaw’s edge, giving a solid grip. The other hand stabilizes the head and secures the temporal bone with the middle finger in the auditory meatus, the thumb and forefinger holding the zygomatic arch, the last two fingers resting on the occiput, and flat palm contact. In this position, the joint is literally held between the two hands (see Figure 7).
To reduce the joint, the practitioner follows the idea of the self-reduction. The movements should be done slowly and with a gentle but directed force. Initially, distract the condylar head by moving the mandible in a caudad direction and maintain the gapping for fifteen or twenty seconds. It may help to think of pushing with the thumb while slightly closing the fourth and fifth fingers, which slightly lifts the front of the jaw. Then traction the mandible forward and toward the opposite side, tracing the anteromedial motion of the disc’s normal motion. The client can help by gently jutting the jaw forward in the same direction, which will help distract the condyle out of the fossa. At the end of the range, the client should relax while the practitioner gently maintains the traction for thirty seconds, making sure that it is not painful; no more distress should be placed on the joint! The practitioner can finish the reduction by gently reapproximating the condyle to the disc (un-gapping the disc space), and holding for thirty seconds. Hopefully, by this point the disc has reduced. Opening and then closing with the teeth meeting tip-to-tip (to ensure that the condyle will still be anterior on the disc) can check the results, being careful not to undo the reduction.
As it happens, just after writing the above paragraph, a client called for a session, suffering TMJ dysfunction. Methodically assessing the situation, I found dislocation without reduction on the left, with soft-tissue spasming stemming from the area of the left mastoid process, along the digastric and stylohyoid to the hyoid bone, and involvement of the entire oral floor to the ramus of the mandible. After releasing the tensions, attempts at self-reduction failed, so the manual reduction was performed and successful. Notable was a “ratcheting” release of tension felt on the prolonged holding of the forward traction phase. Afterward, coaching to maintain a relaxed, anterior “hanging” of the mandible is important, as this will tend to keep the condyle forward, on the body of the disc. Standard dental practice is to combine the manual procedures with an anterior positioning appliance to ensure the appropriate positioning for several days, until the disc and retrodiscal tissues can heal.
As noted earlier, there can be restrictions involved that relate to other paradigms. It is worth mentioning that in this case there was a left cranial torsion present, with the left temporal bone flexed and out of balance with the right temporal in extension, forcing a torsion pattern on the mandible. Obviously, without specific training, this aspect of treatment would be ignored, with the hope that a successful reduction would release the cranial pattern over time.
Allan Kaplan has been a Rolfing practitioner since 1988. He has studied visceral manipulation with Didier Prat, D.O., and assisted him teaching several classes. More recently, he has studied with Jean-Pierre Barral, D.O. and completed osteopathic studies at the Canadian College of Osteopathy.
Bibiolgraphy
Cox, C. 2001 Sept. “Temporomandibular Joint Dysfunction.” Structural Integration: The Journal of the Rolf Institute® 29(3): 22-29.
Murray, G.M., I. Phanachet, S. Uchida, and T. Whittle. 2004. “The human lateral pterygoid muscle: A review of some experimental aspects and possible clinical relevance.” Australian Dental Journal 49(1):2-8.
Okeson, J.P. 2007. “Joint Intracapsular Disorders: Diagnostic and Nonsurgical Management Considerations.” Dental Clinics of North America 51:85-103.
O ks o, J . P. 2 0 0 8 . Maa gmn t o f Temporomandibular Disorders and Occlusion, 6th ed. St. Louis, MO: Mosby-Elsevier.
O ks o, J . P. ad R . dLe u w. 2 0 1 1 . “ D i f frn t i a l D i a go s i s o f Temporomandibular Disorders and Other Orofacial Pain Disorders.” Dental Clinics of North America 55:105-120.
Schwind, P. and S. Schmidinger, 1987. “The Temporomandibular Joint in the Combined View of a Dentist and a Rolfer.” Notes on Structural Integration 1(1):10-19.
Sommer, C. and P. Schwind, 2008 Dec. “The Temporomandibular Joint in the Context of Structural Integration.” Structural Integration: The Journal of the Rolf Institute® 36(4):17-20.
Images from Okeson (2008) used with permission.TMJ Disc Mechanics and Correction[:]