

An old witch from Ranchos told me that La Que Sabe knew everything about women, that La Que Sabe had created women from a wrinkle on the sole of her divine foot: This is why women are knowing creatures; they are made, in essence, of the skin of the sole, which feels everything. This idea that the skin of the foot is sentient had the ring of a truth, for an aculturated Kiché tribeswoman once told me that she’d worn her first pair of shoes when she was twenty years old and was still not used to walking con los ojos vendados, with blindfolds on her feet.
Clarissa Pinkola Estés, Women Who Run with the Wolves
I work a lot on feet. Most of my work is sports-related. I see many hikers, triathletes, and distance runners; mostly amateur, some semi-professional, a few professional. With their feet, I apply Jan Sultan’s Internal- External Model, with some modifications.
Much depends on the relationship between the cuboid and the navicular. Which is up? Which is down? I follow the sometimes-controversial inclusion of the navicular in the transverse arch, as well as the less easily worked upon medial cuneiform. I do this because freeing a superior fixation of the navicular is a good way to relax a high or shortened arch (something I can hardly claim to have discovered). If you disagree with this inclusion, I’ll just have to rely on your tolerance for my idiosyncratic language.
Rotation of the transverse arch in stasis is not the same thing as pronation or supination in movement. Indeed, different demands may produce opposite rotations in the same foot, as in pronation of a high and brittle longitudinal arch that is supinated in stasis. Fairly obvious, but where will I take this? Let’s start with a quote from this article’s epigraph, about “blindfolds on the feet.”
When I analyze a client’s body, I look for blindfolds: lost perceptions, buried possibilities, and unexplored movements I’m seeking what isn’t there, or at least isn’t manifest. Presenting symptoms, pain or weakness or restricted motion, merely reflect the gap between a body’s potential and its present range of perceptions and movements. With few exceptions, our injuries come not from what we did, but from what we failed to do. A runner hurts a meniscus? A yogi subluxates a vertebra? A secretary gets a diagnosis of “carpal tunnel syndrome”? All these injuries reflect over-reliance on one pattern of movement to the exclusion of others. So our work is as much about activating slack muscles as relaxing tight muscles. But the larger goal in both activation and relaxation is to increase options in use patterns, often by addressing antagonist muscles using opposite forms of intervention.
Again, obvious. But “the Devil’s in the details.” In this article I will consider:
What Is a Foot?
So what is a foot? What’s it for? How does it fulfill its function? Yes, the foot mediates the force of gravity in stride, jumping, or other movements. But how? The key is the foot’s ability to react. It responds to various surfaces, of various textures and degrees of hardness, in various directions, at various velocities, in various angles of rotation, supporting various movements of the upper body. Stylistically, I regret this long list. But I must emphasize the multidimensionality of demands placed on the foot. The foot provides a highly nuanced pushback against gravity mediating a mathematically limitless combination of forces. The foot also helps guide ‘anatomy trains’ higher up, often when high speeds or rapid changes of direction are involved.
Perception: The Foot As Sense Organ
But how? Perception. First and foremost, the foot is a sense-organ. Its primary contribution is awareness, then action. More than any biomechanical activity, the foot’s first defining task is to gather impressions and pass them on. Most of the time, feet are our only tactile connection with the usual source of gravity, the ground.
Now I could go all touchy-feely about this, but let’s get specific. I begin with toes. What’s their function? Are they mainly levers? Well, some running coaches still teach a style that overemphasizes the role of the toes in push-off. After all, why else do toes exist? Aren’t they there to mediate gravity at the ball of the foot, the hinge where metatarsals meet the first phalanges? But misuse of this hinge can result in a characteristic ‘bouncy’ stride that wastes energy. Worse, it treats the ball of the foot as a monolithic structure operating in the sagittal plane, disregarding its role in lateral articulation of stress. This is only one example of a mechanistic approach to toes, as if they needed to perform a mechanical function to justify their existence. Instead, let’s look at toes as sensors, as gatherers of information. When I run or hike, I try not to emphasize my toes as levers or pushers or even grippers. (That last is a characteristic temptation for a monkey-footed ‘Internal – more on the Internal/External Model below – like me!) Instead, I let my toes hang fairly loose. I let them act more as antennae. This is entirely different from the ‘lax’ toes of a floppy foot. The toes move, but it is more to seek out sensation than to act as levers.
From Solidity to Open Articulation
But – toes as antennae? What are the practicalities of this? How do perceiving toes change stride? Suddenly, the solid ‘ball of the foot’ becomes the open and articulate ‘toe box’. Force is now articulated more laterally, based on different information going back to each of the five metatarsals. But to achieve this, each toe must transmit its information separately. Toes communicate best in chorus, not in unison. My running coach calls this “playing piano with the trail.”
This looks like a paean to the long, flexible arch and open toes of the Internal. But wait! Too great a reliance on coronal information can dull the equally important perception of sagittal force. The sole of the foot has its own highly nuanced sensors. A long arch with articulate toes will often be clumsy at responding to longitudinal forces. Granted, what’s lacking may be sheer strength in the longitudinal arches and muscles further up. But strength is a product of stimulation: nerves tell muscle fibers to increase their diameters. The sole of the foot has its own tale to tell. Otherwise, why is it so very sensitive?
Even the structures immediately superior to the sole cannot be treated as monolithic, any more than the toe box is monolithic. Specifically, human metatarsals are designed to rotate somewhat independently, even if only slightly. Granted, this movement is inhibited by the need for a relatively firm arch as opposed to that of apes and monkeys. But we have not gone to the opposite extreme of solidity. A dog’s paw is an example of the latter. As a quadruped, a dog apparently does not need the articulation still available to a human foot. Our foot can still grip or push or broaden sagittally or coronally in response to terrain. Specific to coronal movement, a human metatarsal can still rotate somewhat. This is why our metatarsals, cut crosswise, are round, where a dog’s are square, consistent with a less moveable pad. So metatarsal rotations, even slight ones, play important roles in our articulation. Awakening this metatarsal rotation will prove important in addressing restrictions in transverse-arch rotation.
So that’s it. I awaken people’s feet in two dimensions – coronal and sagittal. Only then can I help train the foot to function as a diaphragm, one that spreads or rises asymmetrically depending on situation. This supplies the third dimension. But how does this work? More pertinently, how does it not work?
What Goes Wrong?
Don’t expect a comprehensive list of patterns. Think about it – each bone of the foot is capable of counter-rotating vis-à-vis its proximal or distal partners or its next-door neighbors along the various anatomy trains through the foot. And that’s just bones. It adds up, yes?
For a bone-by-bone, tendon-by-tendon analysis of rotations and counter-rotations (and there are literally hundreds of possible combinations), it’s best to take Liz Gaggini’s biomechanics workshop series. I offer nothing like her detail! At least read her book (Gaggini 2005), The Biomechanics of Alignment, particularly the chapter on arms and legs. I regard it as a must-have. And if you don’t have her latest edition – invest! This article is instead about shortcuts. These work for a high percentage of my clients. But not all shortcuts pan out. When that happens, I pull out my ten years of heavily-annotated Gaggini books.
The Internal-External Model and Movement Temptations
I start off with Jan Sultan’s Internal-External Model. For those unfamiliar, Internals tend to be varus or ‘bowlegged’ in the knees, with bulging occiputs, relatively high-amplitude spinal curves, and generally long and flexible arches. Externals have valgus or ‘knock-knees’, flatter occiputs, and lower amplitude spinal curves – though sometimes sporting an impressive kyphosis. Their arches are likely to be short and rigid, though I have seen well-functioning short arches on Externals. (By the way, I prefer to pair the terms ‘long’ and ‘short’ rather than ‘long’ and ‘high’, but don’t read too much into that semantic difference.) This is quite simplified, but I hope it’s enough. Now I take Internal-External ideas down some odd paths (so don’t blame Sultan). On the other hand, I cannot claim with certainty that my insights are entirely new; I surely repeat what others have presented.
Some Internals have short arches, while some Externals have long arches. So I ask: “Is a short arch on an Internal identical to the short arch more commonly found on an External? And is a long arch on an External identical to the long arch on the average Internal?” Not at all. So why – and how – do these arches differ? One possible explanation may be found in Sultan’s model of Congruent Internals and Externals vs. those not congruent. Feet and/or lower legs rotate either congruently or not with the humeri. But I confess that I have not studied this model and its bearing on foot problems. Instead, I present a model that has little to do with such rotations, relying instead on movement patterns existing within feet themselves. This is not to say that Sultan’s typology and mine are incompatible. Nor do I claim that they are totally . . . congruent.
Here’s my take: Internal-External patterns exist within feet in what I call ‘movement-temptations’. These are the movements that ‘feel right’ and are relatively ‘easy’ for a client. Regardless of the length of the arch, these movement patterns remain fairly consistent with Internal-External type. This correlation has profound implications for customized treatment. Briefly, the movement-temptation of the Internal foot is coronal, with the cuboid usually stuck relatively superior in relation to its nearest neighbors, though situational supination is not impossible in such a foot. The movement-temptation of the External foot is sagittal, with the navicular usually stuck up, though pronation is possible under stress.
Arch-Length Typology
But how does this translate into different lengths of arches? I start with the usual Internal-External types, expressed in long and short arches respectively, then move on to the countervailing types whose arches go against this pattern. Let me repeat that this typology does not include all clients. Here goes.
Long-arch Internal

Figure 1: Long-arch Internal, lateral (A) and superior (B) views.

Figure 2: Long-arch Internal, posterior view, client prone.
Our first type is the Long-arch Internal. See Figure 1 for two views of a long arch. Viewed laterally (A), note the lack of angle at the end of the metatarsals, indicating relaxed toe extensors. Toe spread is generally wide (B). With the client lying prone with feet off the edge of the table, there is often a paradoxical supination of the transverse arch (see Figure 2). Manual rotation of the mid-foot often produces some pronation. But supination reveals a stuck-up cuboid. This means that the fifth metatarsal cannot freely rotate downward relative to the fourth one, so that the role of the adductor digiti minimi (ADM) is restricted in its underreported longitudinal motion, which is what makes this muscle such a vital part of the lateral arch. However, the strength of the Long-arch Internal is that toes are able to move laterally with relative ease. Specifically, the ADM can contract in its usual namesake movement with little practice, even in a client who has previously never experienced this movement. How do we test for this? First, determine which foot is dominant: “Which foot would you kick a ball with?” Then have the client spread the toes laterally. With short longitudinal arches, toe extensors often take over the movement, lifting the toes as a block, which means that you may have misidentified the client. However, with clients who simply possess poor proprioception, another way to assess for a Long-arch Internal is to lie the client face down with feet off the edge of the table. Paradoxically – and I don’t quite know why – feet that pronate in stasis will often supinate in this position; something to do with the actions of muscles inferior to the lateral malleolus. All I know is that this sometimes works. What we’re looking for is preponderance of evidence, not a single definitive sign. Bottom line: a foot that can access ADM contraction, even if it takes some practice, will almost certainly have a genuinely flexible long arch, which is not the same as a fallen or slack arch, which we’ll see later.
Short-arch External
Our next type is the Short-arch External. In Figure 3 we see the short arch viewed laterally (A) and a relatively closed toe box (B) with incipient bunion. With the client lying prone with feet off the table, often there is a paradoxical ‘flatness of the arches, as seen in Figure 4. (Warning: this is not always the case!) But manual rotation of the mid-foot generally produces supination and little or no pronation. In client-generated movement, the ADM contracts only with much practice and hands-on work. The ‘tyranny of the big toe’ predominates, overruling the direction and overall perception of the other toes. If anything, short extensors will lift the toes up en masse, as noted above. This involves the characteristic stuck-up navicular and stuck-down cuboid. In turn, this supination of the mid-foot favors a characteristic ‘peak’ at the meeting place of the proximal first and second metatarsals. So as with metatarsals four and five in the Long-arch Internal, we have two metatarsals unable to rotate freely versus each other. But here, the first metatarsal is larger, more robust, and more apt to dominate movement. But this client will often report pronation in running. Supination of this foot is unsustainable due to lack of lateral movement in the toe box. And once again the paradox presents itself – with the client lying face down with feet off the edge of the table, feet will often appear more balanced in transverse arch rotation. Sometimes this is a result of the legs being spread far apart; feet closer together often appear more supinated in this position, as in the Long-arch Internal. So this is not entirely reliable. Again, we are looking for a preponderance of evidence.
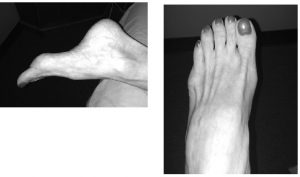
Figure 3: Short-arch External, lateral (A) and superior (B) views.

Figure 4: Short-arch External, posterior view, client prone.
Short-arch Internal
There are no photos for the remaining types. This is because visually these conditions often present like their opposites in the Internal-External Model.
Next is the Short-arch Internal. Visually, this client often presents like a Short-arch External, and indeed, in manual rotation at the mid-foot, the problem may initially present as similar with a stuck-up navicular.
But check the cuboid! Can manual rotation produce supination? And in a sidelying position with pressing, can the cuboid or metatarsals four and five go anatomically inferior vs. the lateral malleolus? In the Short-arch Internal, generally not, so one mechanism of an external-type short arch is missing. Why? In my practice, most Short-arch Internals are women who have worn high heels. The toe-box generally forms an incipient or fully developed bunion, often unilaterally. The toe-hinge is usually stuck in something close to a 90? angle by the extensors. But the good news is that this compressed toe box often hides an ADM that, with a little practice, develops robust movement. But watch out for fake Internals! Feet that don’t fit the Internal-External pattern may indicate that disorganization is even deeper and more pervasive than my little shortcut indicates. Unilateral or bilateral internal femoral rotation combined with valgus knees indicates somebody even less functional than a Short-arch Internal. In my experience, this combination of traits often manifests deep shame and fear – in either gender.
Long-arch External – Slack
Now we look at the Long-arch External – Slack. Manual rotation often produces loose pronation and supination in a slack foot, but more supination even with this slackness. This client tends to have feet with little muscle tone or nerve flow. Floppy, with little active spreading, extension, or flexion of the toes. The leg stance is often especially far apart, and gait has a characteristic waddle. But watch out for fake Externals! Here the problem often involves a fixed posterior sacrum – resulting from poor martial arts training, incompetent structural integration, or both. I wish I had a nickel for every time I’ve seen a pointy-occiput Internal with bowed legs, flaccid glutes, a gorilla-like kyphosis, and a story of having been “fixed” by a “Rolfer.”
Long-arch External – Fallen
The last type is the Long-arch External – Fallen. Here manual rotation tends to produce results like a Short-Arch External: more supination than pronation. Good news is that the cuboid remembers how to rotate down. This is just a fallen short arch. Extensors are exhausted, but possess muscle memory. Curiously, this kind of foot has often developed good ADM ability in response to its collapse. I often find such feet to involve intelligent efforts by the body in middle age to respond to an earlier fixed, short arch.
What to Do . . .
Like the previous section, this is not comprehensive. But now I am even more restrictive: I list only one (or two interrelated) interventions for the above types, with subcategories for Hands-On and Homework. This is plenty. And all, this is limited to the relation between the toes and the transverse arch. So please don’t approach feet with only these few tools. Fit them into your toolbox.
To begin: I described the movement-temptation of the Internal is coronal, that of the External as sagittal. The trick is to awaken the counterintuitive movement pattern without surrendering the default pattern. This creates a foot that moves in all three dimensions. But this involves integrating the default movement pattern so that it no longer excludes the missing dimension. The primary pattern generally requires further refinement to play its role in supporting the one newly accessed. I don’t just add the missing dimension, lest the foot become even more disorganized than it was.
For example, the ADM of even a fairly well-organized Internal often doesn’t know how to work independently of the middle three toes. It pulls all these toes away from the hallux in a fanning motion. Great for analysis, but now I must help the ADM to work independently. I’m looking for abduction of the little toe with relatively little movement of the middle three toes. Not easy! But as I mentioned, a truly independent ADM is better equipped to play its secondary (if it is secondary) role in the lateral arch.
. . . For the Long-arch Internal
Hands On: As noted above, the Long-arch Internal usually has a stuck-up cuboid. But the navicular is not especially mobile. If one is stuck, both are almost always stuck. So I go back and forth, testing and working. I rotate the navicular on its long axis manually, testing and freeing it proximally and distally. But unlike a stuck-down cuboid, a stuck-up cuboid requires work on the superior more than inferior side. I must free the fifth metatarsal to rotate down vis-à-vis the fourth. I hold the fifth metatarsal laterally and explore space between four and five, wriggling the held metatarsal to create space and articulation. I also sculpt distally along that four-five intersection till I get to the mid-foot. Then a stuck-up cuboid may respond to broader-hand moves with the client in the Third-Hour position. On the foot whose outer edge faces upward, I press distally along the lateral edge so that metatarsals two to four all move toward supination. I can then push laterally across the junction of mid-foot and metatarsals to reinforce that rotation.
Homework: Longitudinal arch-building is key. But getting up on the toes is only one method. And that kind of exercise will cause problems without other feedback, creating secondary patterns instead of fixing the first one – including overuse of the toe-hinge in gait. But all human feet are innately prehensile, yes? So an Internal, who has articulate toes, can recruit that ability to the task of plantar-flexing with toes pointing. I ask the client to pick up smaller and smaller things. Warning: picking up ten quarters can cause hideous cramps – try it! Maybe start with something bigger and softer, like socks. But as I mentioned above, also expand the independence of the ADM in lateral movement.
. . . For the Short-arch External
Hands On: For the Short-arch External, the stuck-up navicular is a given. But in addition to freeing its ends, I ‘undermine’ the metatarsal restriction closest to the navicular. As noted, independent lateral toe movement is often difficult for this type. As mentioned above, a central aspect of this type is the tyranny of the big toe. Fortunately, there is a similarity to treatment of the Long-arch Internal: creating independent motion between adjacent metatarsals. The difference is that here, the metatarsals to be separated are one and two, rather than four and five. I hold the metatarsals apart and wriggle them. From the superior side, I work proximally along this gap till I reach their meeting point (warning: very sensitive spot!). But a fixed short arch is quite susceptible here to change if loosened by metatarsals starting to move independently. This is more challenging in clients who wear flip-flops, as this gap does not represent independent movement, but rather a dead zone of slack tissue and unresponsive nerves.
Homework: As noted, a Short-arch External often takes a while to access the ADM, so the abduction movements are key. But the toe box often can’t open because it’s stuck at an awkward angle by tight extensors. So I want the toes to flex, yes? But a short arch generally involves tight flexors. So instead of picking things up with toes, I encourage clients to Plantar Flex their toes passively. I have them sit seiza – sitting on their knees on a flat surface with the feet tucked under and toes passively flexed (see Figure 5.) Better that extensors release than be overruled by already-overworked flexors. But as seen in Figure 6, it is important to keep the feet straight (A) instead of touching the big toes together (B) as Japanese people often do. We’re not doing tea ceremony! A seiza bench might be necessary for starters. As the cliente is able to go lower down, one can use a rolled up towel under the anterior ankles. But the goal – in terms of what supports the ankles – is to have nothing there.
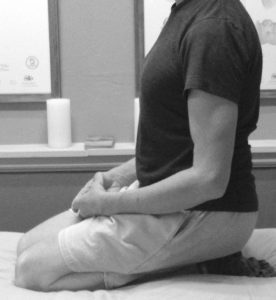
Figure 5: Seiza posture, side view.

Figure 6: Seiza posture, correct toe placement (A) and wrong toe placement (B) for our purposes.
. . . For the Short-arch Internal
Hands On: Work on the medial and lateral metatarsals is more balanced than in the first two types. With this type, both sides of the toe box contribute more equally to the problem – and to the solution. Articulate abduction is usually an innate strength of the Internal foot, however stifled by bad shoes. The fourth and fifth metatarsals must separate to allow this, but with a little loosening, the ADM is often raring to go. With the foot finally experiencing its innate lateral movement, it’s time to strike at the main buttress of the short, high arch by separating metatarsals one and two.
Homework: As with hands-on work, I seek a balance of work suitable to the first two types, but the reason is somewhat different. In this type, feet are often especially traumatized by bad shoes. Despite innate strengths, these clients may experience difficulty doing any movements at all. So I must explore a greater repertoire before we find something involving relatively little pain and frustration.
. . . For the Long-arch External – Slack
Hands On: If hands-on work is just an introduction – and invitation – to the homework, this is especially so for slack muscles. Here, manual work is more about awakening sensation than moving tissues. Granted, perception ought to be a key part of every intervention, but here it’s dominant. A passive rotation of the transverse arch can be a game-changer for the client: “Whoa, this moves?”
Homework: For the Long-arch External – Slack, I contradict my earlier critique of walking on toes: there’s little danger of the toe-hinge being overused, or of an excessively bouncy walk. (Have you ever seen a slack-footed client shuffling along with heels barely half an inch off the floor?) And this seems to yield better results than just standing in place lifting the heels up and down. But in a pinch I’ll start with that.
. . . For the Long-arch External – Fallen
Hands On: As with a Short-arch Internal, I balance work on the medial and lateral metatarsals. Again, I seek independence of two pairs of metatarsals: one vs. two and three vs. four. But with this type I suggest less manual work, more movement.
Homework: Again there’s a similarity to the Short-arch Internal: I try out a relatively large repertoire of range-of-movement exercises, but here the reason is the exact opposite: unlike Internals with severe damage from high heels, these clients often have sophisticated feet with multiple strategies for dealing with the changes they are undergoing. For example, such clients usually address increasing pronation by opening up the toe box, but without sacrificing appropriate mobility of the cuboid. But this sophistication is usually unconscious.
Conclusions – What About the Rest of the Body?
I have deliberately left loose ends throughout this article. Clearly, neither my typology nor my interventions can stand alone – pun intended. For one thing, feet and lower legs cannot really be addressed separately. Just one example: I find that a fixed short arch often responds to work at the tibialis posterior right at its most superior insertion, whatever restrictions I may palpate along septa further down. But I cannot possibly add a section outlining all such implications!
Still less am I able to address the coronal vs. sagittal ‘movement temptations’ in the feet of Internals and Externals as they interplay with the rest of the body. Is there, for example, any relationship between the ‘coronally tempted’ toe box of the average Internal and this person’s ability (if healthy) to use the spine like a contracting and expanding Slinky®? I’m inclined to think that there is a common theme of agility here. On the other hand, is there any connection between the ‘sagittally tempted’ arch of the External and his ability to bear weight with a relatively straight spine? Again interesting, but both these speculations are far beyond the scope of this article.
So that’s it. You’re on your own. Have fun, try stuff out yourself, wriggle your toes, climb things, grow a tail, live three-dimensionally, wake up your inner Happy Monkey and Wise Ape, deepen whatever Internal-External pattern is natural to you, explore whichever pattern feels counterintuitive, find where the two patterns intersect. And if you feel like it, drop me a line.
Michael Boblett works in San Diego, California. He has been a Certified Rolfer since 2003 and a Certified Advanced Rolfer since 2008. He is a retired Unitarian minister. His advanced degrees (MA, MDiv, and DMin) are from Pacific School of Religion in Berkeley, California. At seminary, his focus was on the anthropology of religion, with experiential training in shamanism under Michael Harner, author of The Way of the Shaman.
Bibliography
Gaggini, L. 2005. The Biomechanics of Alignment, Sixth Edition. Self-published, available at http://connectivetissue.com/ publications.The Three-Dimensional Foot[:]