

Introduction
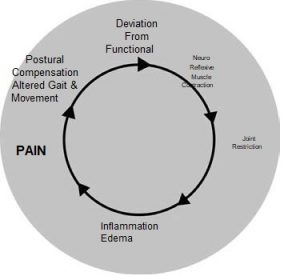
Movement restrictions in the joints of the axial skeleton produce an immediate alteration in the client’s structure. These alterations can include such patterns as leg-length discrepancy and changes in pelvic inclination as well as orientation of the spinal curves. They also produce localized inflammation and edema, which is experienced by our clients as pain. Arrays of compensations are then developed in an attempt to reduce that pain. These compensations can develop throughout the body. At this point, the client’s structure is dramatically altered (see Figure 1).
The assertion of this article is that quickly identifying and mobilizing axial joint restrictions will greatly expedite the goals of structural integration (SI). Although this is a ‘post-Ten’ case study, these types of compensations can complicate any session of a series. For example, the simplest of sacroiliac restrictions will produce a leg-length discrepancy, which will completely alter foundational support and grounding. A lumbar facet that will not extend locks the vertebra in flexion. This can flatten the lumbar curve and tilt the pelvis posteriorly. It is easy to see how these two compensations would effect a Second, Fifth, or Sixth Hour of the Ten Series. As will be demonstrated in this article, when these restrictions are mobilized, many of the compensation patterns quickly resolve. Without taking joint restrictions into account, a practitioner can waste valuable time and even an entire session chasing the wild geese of compensations.
Background
During my advanced Rolfing® SI training in 1989, I was introduced to the world of spinal mechanics. I quickly saw that this was going to radically change and deepen my understanding of SI. Spinal mechanics can easily become complicated and confusing. I found myself spending more time trying to figure out what was going on with my client’s spine than actually working. I realized that I needed to find or develop a tool to quickly organize specific assessments and procedures that would bring order to the chaos and expedite that phase of a session.
In emergency rooms (ERs), where speed and accuracy are essential, algorithms are used in the delivery of care. Health-care algorithms are analytic tools derived from evidence-based criteria. They are used to improve quality of care by increasing the accuracy and specificity of assessment and treatment while also saving valuable time (Iyengar 2009). Inspired by my work in the ER, I combed the literature for information, broke it down into digestible chunks, and applied the principles of SI to what I found.
The Lumbar-Pelvic Algorithm is designed to expedite the specific identification and resolution of joint restrictions in clients with complications in the back and lower extremities. By following the algorithm, a practitioner is able to quickly assess axial joint function without being an expert in spinal mechanics.
Procedure
The algorithm begins with a simple movement test, which has a clear positive or negative result. The result directs the practitioner to a specific palpation test, which identifies the joint restriction. The algorithm then leads to a procedure that will resolve the restriction. Then the movement test is repeated to assure freedom of movement in the joint (see Figure 2 for an example based on a section of the Lumbar-Pelvic Algorithm). The algorithm assessment process takes only about three to five minutes, and if no positive results are found the practitioner is assured that joint restrictions will not interfere with accomplishing the session goals.
This algorithm is divided into three sections: foundation, mobility, and locomotion. The progression of the algorithm applies the following principles: foundation precedes mobility, and mobility precedes locomotion. The foundational section assesses the pubic symphysis function and up- or down-slip of the innominates. These joints connect the axial skeleton to the lower extremities and the ground. Stability in these joints is essential to the function of the rest of the lumbar and pelvic regions. These assessments are also often confused, so the algorithm guides the practitioner through a differential assessment. Next, in the mobility section, restrictions in the lumbar spine are assessed and addressed. Once the lumbar facets are functional, the algorithm leads into sacral assessment and intervention. Since the rotation of the innominate on the sacrum is essential for proper gait, the locomotive section assesses and treats innominate rotation restrictions. As you proceed through the algorithm, each intervention supports the next, so there is no need to repeat a test or procedure.
Muscle energy technique is used as the intervention. This technique was developed by Fred Mitchell Sr. DO in the 1950s. It is an intrinsic technique in that the activating force is an isometric contraction completely controlled by the client. This contraction stimulates reflexes that temporarily override the reflexive muscle contraction restricting the joint. During the seconds in which the restrictive muscles let go (post-contraction reflex), the practitioner gently moves the joint into its functional range of motion. Since the procedure is gentle and uses the intrinsic force of the joint-stabilizing muscles, the client’s body does not have to negotiate the forces of high-velocity low-amplitude adjustments.
Case Study
With this background, we can now proceed to the case study.
Client History
Our model is a forty-year-old female yoga two years earlier. In the interview, she complained of right-sided low-back pain. She described her pain as radiating around her right iliac crest to the anterior superior iliac spine (ASIS) as well as the back of the right calf and ball of the right foot.
Pre-Session Standing Assessment
The client stands with knees locked and weight over her heels (see photo A in Figure 3). She has an anterior pelvic tilt, and an exaggerated lumbar lordosis. The rhomboids are in a hypertonic state, decreasing the thoracic curve. Her shoulders are elevated and the head is drawn forward. There is a high level of tension in the jaw.
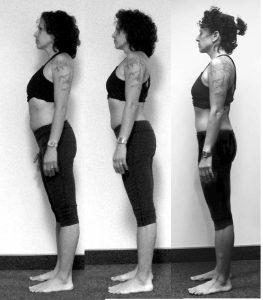
Figure 3: A – pre-session; B – mid-session, post-algorithm; C – post-session.
Pre-Session Gait Analysis
As the client walks, she bears the majority of weight on her left leg while avoiding weight on the right leg. The left leg is externally rotated while the right leg is slightly internal. She lifts her right leg from the waist, over-engaging her right quadratus lumborum. There is no contralateral movement between upper and lower extremities. See video clip at http://tinyurl.com/nvpgb7l.
Applying the Algorithm
The algorithm starts with a standing flexion test (see Figure 4; deMahy 2013) to assess for dysfunction in the foundational joints of the pelvis. With a positive finding, the position of the ischial tuberosities on the horizontal plane is used to differentiate between superior innominate (up-slip) and pubic-symphysis dysfunction.

Figure 4: Standing Flexion Test: the test
is positive if one PSIS moves anterior and
superior before the other.
The client had a positive finding on the right side in the standing flexion test. Palpation revealed horizontal ischial tuberosities, ruling out innominate up-slip. Palpation of the pubic symphysis revealed a right superior pubic symphysis. The symphysis was treated and then retested. The negative result of the test showed that the intervention had been effective.
Next we test for axial mobility, comparing the lumbar spine in neutral prone to its position in extension and flexion. The rotation of L5 did not change in extension, indicating functional movement. However, in the flexion test L5 rotated right as compared to neutral. This signifies that the right facet would not open during flexion, i.e., a right L5 flexion restriction. L5 was then treated (see Figure 5; deMahy 2013) and then retested with a negative result.

Figure 5: Client positioning for lumbar
flexion restriction procedure.
The algorithm then moves into the sacral section (Figure 2), using the seated flexion test (Figure 6; deMahy 2013) to assess for the presence of sacroiliac (SI) dysfunction. As the client’s lumbars flexed, the right posterior superior iliac spine (PSIS) was quickly dragged up by the spine, indicating a right SI dysfunction. With the client prone, palpation revealed the right sacral base was anterior and the right inferior lateral angle of the sacrum was posterior and inferior, which identified a unilateral right anterior nutated sacrum. The sacrum was treated and then retested with a negative result.

Figure 6: Seated Flexion Test. Like the
standing flexion test, this is positive if one
PSIS moves anterior and superior before
the other. When the legs are taken out of
the equation, flexion exhibits the function
of the sacrum on the ilium.
Now that we have mobility of the lumbars and sacrum, we assess the movement of the ilia on the sacrum. The Stork or one-legged standing test (see Figure 7; deMahy 2013) is used to assess the presence and side of this dysfunction. With this client, the test indicated a right iliosacral dysfunction. By comparing the levels of the ASISs and PSISs, the client exhibited a right anterior innominate rotation. She was stuck in the push-off part of the gait. The iliosacral joint was treated (see Figure 8; deMahy 2013) and then retested with a negative result.

Figure 7: The Stork Test is positive if the
PSIS moves superior in relation to the
sacrum.

Figure 8: Client positioning for anterior
innominate rotation procedure
At this point, twenty minutes into the session, the algorithm was completed. As displayed in the after algorithm photograph (see Figure 3, photo B), many of the compensations have been resolved, clearing the floor for the rest of the session. The client stands with her knees unlocked and her pelvis near horizontal. There is a decrease in rhomboid tone and her thoracic curve has returned. Her shoulders are resting down, her head is nearly over her shoulders, and there is a marked decrease in jaw tension.
Post-Algorithm Gait Analysis
Contralateral movement has been restored and weight bearing is bilateral. The rotation of the legs is now bilaterally symmetrical. The right quadratus lumborum has released, restoring normal swing in the hip. See video clip at http://tinyurl.com/l4rfz89.
The Rest of the Session
There is still forty minutes left in our hour-long session. With many of the compensation patterns out of the way, the job of stabilizing and integrating her structure is well on its way. Here I am looking at how to increase support in her feet and legs, equalize movement in the pelvis, decompress the lumbars, and bring those changes up through the head.
These goals were accomplished (see photo C in Figure 3) through the following steps:
Client Education
Knowledge gives a person power over her pain by decreasing anxiety and increasing body awareness. Client education includes explaining each restriction and how it contributed to her pain. In this particular case, we discussed the importance of a stable and mobile pubic symphysis. Although she did not feel pain in the front of her body, dysfunction at the symphysis was most likely the beginning of her problem; it changed the length of one leg and altered the range of motion of the same-side SI joint, causing a domino effect through the rest of the pelvis and low back.
The most common cause of a right superior pubic symphysis is stepping off of a curb and landing on a straight right leg. The jolt up the leg stimulates the neuromuscular reflex to lock the joint. More relevant to this client, this dysfunction can also be caused by aggressive yoga practices. Attempts to stretch the adductors can lead to stretching the ligaments of the symphysis. It is important to strengthen the secondary stabilizers of the symphysis, which are the muscles of the transversus abdominis and the anterior pelvic floor. Considering her yoga background the mula bandha and uddiyana bandha were recommended.
Conclusion
The use of algorithms is in no way intended to replace the invaluable process of ‘seeing’. However, this case study does demonstrate that the use of an algorithm and joint mobilization can greatly enhance and expedite the process of integration. The use of algorithms is useful not only in post-Ten sessions but throughout the Ten Series. In Rolfing SI, fascia is where we dance, but if there is glass on the dance floor, doesn’t it make sense to sweep the floor first?
Bibliography
deMahy, J.R. 2013. Joint Restriction in Structural Integration, Vol. 1, 4th Edition. Self-published.
Greenman, P.E. 2010. Principles of Manual Medicine, 4th Edition. Baltimore, Maryland: Lippincott Williams & Wilkins.
Iyengar, M.S. 2009. The Medical Algorithms Project. http://arxiv.org/pdf/0908.0932.pdf.
Mitchell, F.L., Jr. 2004. The Muscle Energy Manual Volumes 1-3. East Lansing, Michigan: MET Press.Joint Restriction in SI[:]