

ABSTRACT The author discusses an approach to low-back pain and pelvic asymmetry that looks at nerve tethering as the pain generator. He discusses a manual approach to repositioning nerves and fascia to release nerve tension.
Most clinical approaches to low-back pain focus on the condition of the intervertebral discs and impingement of spinal nerve roots. Idiopathic low-back pain is not explainable according to the standard diagnostic tests and imaging. The primary references in mainstream literature offering explanations other than the intervertebral disc for back pain derive from a doctor Robert Maigne (1989, 1991), who specifically suggested that lumbar dorsal rami can also contribute to back pain. He suggested that the dorsal rami of the lumbar vertebrae, aka cluneal nerves, can be main contributors to back issues. The main allopathic medical treatments include steroid injections, disc surgery (sometimes unnecessarily), spinal fusions, nerve blocks, and opioids. It seems none of these really address what is frequently a major cause, which in my experience amounts to a sagging and tension on multiple nerves at once. This scenario should be examined particularly in clients whose MRIs show no apparent disc involvement.
Recently, our colleague Robert Schleip and coworkers have also suggested that nociceptors in the lumbodorsal fascia can be the source of low back pain, as evidenced by increased numbers of myofibroblasts and other inflammatory mediators (Wilke et al. 2017). In addition, I agree with Maigne and suggest that as a source of idiopathic low-back pain we extend our consideration beyond the lumbodorsal fascia to the perforation sites for the cutaneous dorsal rami (and the other components of the neurovascular bundles), as well as a collective tension on several nerves, particularly segments of the lumbar and sacral cluneal nerves where they cross the iliac crest, sacroiliac joint, and hips, and to include their entire pathways plus skin innervation. If the entire course of a nerve is not free to glide and stretch evenly, it potentially could lead to tension on the vulnerable segments or branch points and, ultimately, on the nerve root and spinal cord. This can drive neurogenic inflammation. The documented evidence of nociception by nerve-sheath nervi nervorum (Sauer et al. 1999) would suggest that pain and neurogenic inflammation could be generated anywhere along the nerve sheath of any peripheral nerve by mechanical stretch.
As Rolfers, we tend to look holistically at broader fascial strain patterns and structural distortion. Taking a more neurocentric perspective than our normal way of looking at fascial strain patterns, it makes sense to look at the strain patterns within or along the larger neurofascial tree in the more distal peripheral tissues, because tensional forces on nerves can be a large driving force for inflammation and pain, as well as the inhibition of muscles that limits mobility and prevents further damage. Addressing the strain patterns in the peripheral nerves themselves is key to attain the kinds of structural results that we want and successfully treat people with low-back and hip issues. In many cases, the tension on superficial cutaneous nerves may be as important as any deeper myofascial and neurofascial structures in contributing to pain, poor range of motion, joint stiffness, and immobility. I suggest that one major focus should be to reposition the fascia to relieve strain on the nerves.
A previous article (Evanko 2010) discussed generally how the superficial fascia and the nerves therein are underappreciated for their role in postural distortion and movement patterns. Our colleagues, the late Don Hazen, as well as Robert Schleip, Christoph Sommer, and Jon Martine have been inspirational along this avenue. Hazen popularized the idea in our community that tethering by fibrous connective tissue (fascial bonding) around the nerve sheaths creates susceptible places where the nerves can be overstretched and sensitized. Restoring lateral and longitudinal glide for the nerve, as well as flossing and extensibility of nerves, is emphasized. Dampening inflammation by mobilizing inflammatory exudate around nerves, with light pumping action, was also emphasized by Hazen. Barral and Crobier (2005) have an excellent book on the theory behind and techniques for direct nerve manipulation. This article will discuss specific, but broader strain patterns within the nerves and superficial fascia that may give rise to back and hip pain, and their role in pelvic asymmetry.
What are the consequences of sagging, twisted, and bunched superficial fascia and deeper investing fascias? The basic answer is that it places tension on multiple peripheral nerves. As Hazen pointed out, the nerves tend to rule everything, so more focus on their role in creating or holding the patterns we address in a structural integration series is important.
Research (Sauer et al. 1999) has shown that mechanical irritation (such as a stretch) or other noxious stimulation of spinal nerves and sciatic nerve preparations can result in the release of nociceptive neurotransmitters from the nervi nervorum within the nerve sheath. In addition, the nerve sheath, whether it be the nervi nervorum or the fibroblasts, can be the source of inflammatory mediators, such as prostaglandins. This is the basis of neurogenic inflammation, which also includes antidromic activity (weak electrical activity out of the spinal cord and down sensory nerves) and the transport of inflammatory mediators to the tips of the sensory nerves. This means that the nerve sheath itself can act as a sensory organ, with the nervi nervorum, or other types of stretch receptors, such as Ruffini endings, monitoring the tensional state of the nerve. Tension on the nerve sheath can result in motor inhibition and/or pain. An acute over-stretch of one or more nerves can result in ectopic firing, electrical zingers, and spasms that can mimic a disc ‘going out’ (speaking from personal experience when my own back went into spasm, when my belt and tight waistband raked across my iliac crest and my already sensitive iliohypogastric nerve was violently jerked by ill-fitting jeans and belt).
Torsional patterns within the superficial fascia and in the deeper investing fascias are underappreciated, and untwisting the rotations in the myofascia can be key to mobilizing the nerves in the legs and thigh. We’ve all felt how the fascia lata and deeper muscular structures can be laterally rotated at the hips. This will tend to put a twisting strain on the nerves that cross the hips. Further down the legs, there will be with twists in the crural fascias and associated nerves. Similar torsion (but typically internal rotation) occurs in the fascia and nerves of the shoulder girdle and arms.
Sometimes palpation by skilled hands is superior to currently developed imaging techniques. While expensive MRI imaging or ultrasound can sometimes detect inflammation around nerves at local peripheral sites, imaging techniques would likely be unable to reveal longitudinal tension along a small segment, let alone the entire pathway of a nerve. There may also be low-grade inflammatory processes, or neuritis, happening that is below the resolution of the imaging technique, but that skilled palpation can detect.
Careful palpation reveals the broader strain patterns and tension along many neural pathways as they course from the spinal cord through various muscle layers and fascial or bony tunnels, and then perforate into the superficial fascia. This will include tension along various branches that terminate in the skin. Basically, tension along the skin is a good indicator of tension along the cutaneous nerve. Knowing the pathways of the nerves and being able to palpate strain along them will help Rolfers to be more effective in addressing structural issues and avoid potentially creating inflammation by inadvertently overstretching nerves as we work.
Figure 1: Posterior cutaneous nerves involved in low back and hip issues. A – nerve anatomy adapted from Netter (1989). B – the lateral and downward pull of the superficial fascia is shown. C – directions for repositioning fascia and nerves.

Figure 1 illustrates the posterior cutaneous nerves (A) and the direction of strain (B) that is common in difficult-to-explain back issues. These nerves and the fascia containing them tend to be pulled down the buttocks and legs and their proximal segments (from the perforation site in the investing lumbodorsal fascia layer and across the iliac crest) are subject to overstretch, like little rubber bands. The tethering can extend farther down the glutes or the leg than one might realize.
As mentioned above, the iliohypogastric nerve (see Figure 1) can be very much involved in back issues. This nerve comes from the ventral ramus of L1 with some fibers from T12 and travels through the body wall, with a lateral cutaneous branch emerging through the external oblique muscles near the lumbar triangle of Pettit, next to the quadratus lumborum muscle. The cutaneous portion passes inferiorly behind the greater trochanter where it is usually tethered in the dense fascia. It also has a vulnerable branch point, just superior to the iliac crest. The anterior branch travels forward along the inguinal ligament. This nerve is often the source of trouble when back pain complaints also involve pain radiating down toward the pubes. The branch point in the back is quite susceptible to pulling as the anterior branch sags over the top of the inguinal ligament with the rest of the belly and the posterior branch sags down the hip (see Figure 2).
Traveling further toward the sacrum, we run into the superficial lumbar (or superior) cluneal nerves, which tend to be tethered over the gluteal muscles, as well as the middle cluneal nerves or the sacral cutaneous nerves, which emerge from the sacral foramina and get tethered in the sacroiliac ligament and also over the gluteal musles [Figure 1 (A)]. All of these nerves tend to get pulled downward by sagging due to gravity and, especially, when seated in a slouching posture that creates a downward drag on the superficial fascia and gluteals. Of course, the gluteal nerves (not shown) are deep to the gluteal muscles and will also be involved. All the tissues here, including gluteal fibers, need to be unrolled and lifted in a headward direction. A strategy that frees the entire course of the nerves and feeds them back toward their origins and spinal cord works well [see Figure 1 (C)]. Attention also has to be paid to differentiating individual dermatomes as well, because adjacent patches of skin can be innervated by a nerve from front and one from the back. For example, the dermatome of the lateral femoral cutaneous nerve can encroach on the tissue supplied by the posterior femoral cutaneous nerve and care along these lines can pay off.
Another nerve that I find very important in back pain is the posterior femoral cutaneous nerve (Figure 1). The superficial strain on the nerve is not appreciated much either because tension on this nerve is often confused for hamstring tightness. It emerges near the hamstring tendons by the ischial tuberosity and travels superficially down the back of the leg in the fascia lying over the hamstrings, and then terminates below the knee. Sagging of the superficial fascia here puts a great deal of strain on this nerve. So, with respect to pelvic asymmetry, on the posterior tilted side, tight hamstrings and sagging gluteals come with a more superficial level of tension along the posterior femoral cutaneous nerve and pulling in of the fascia along its branches. If you palpate carefully you can feel how the superficial fascia is usually gathered up around the knee (and also the ankle) like bunched up stockings. Careful attention to spreading out and moving the superficial tissue superiorly (or headward) to take the strain off of the nerve is important. It is also very important to work to differentiate at the gluteal fold and to lift the glutes off the leg. In some people the glutes are halfway down their leg, putting tremendous collective strain on all the posterior nerves. Extended sitting, especially on toilet seats, is one way in which the posterior fascia lata and the posterior femoral cutaneous nerve can be repeatedly dragged down the legs.
More deeply, the sciatic nerve (not shown) tends to get tethered deep to the gluteal insertion on the IT band and, of course, in the lateral rotators and beyond. Tethered and twisted branches of the sciatic that innervate the hamstrings can be responsible for cramping when overstretched or torqued by muscle action. This means that deeper into the back of the leg we must make sure that the hamstring fascias, which get rolled and adhered to each other (mostly from sitting) are well differentiated also. Aim for fluidity in the seams between investing fascias, where the nerves travel. The common peroneal nerve (not shown) is almost always tethered along the tendon of the biceps femoris and around the knee and the fibular head. Judicious use of fingernails to gently pick the nerve loose from the tendon is effective. Releasing the common peroneal nerve is vital in a posterior tilt pattern. The extensibility of the tibial nerve all the way down to the foot and plantar nerves should also be assessed and will affect lower leg cramps.
In order to relieve pain most effectively all the superficial (and deeper tissues) essentially need to be repositioned headward to take the strain off of these nerves [see Figure 1 (C)]. Special attention may need to be paid to dampening inflammation around particularly tender nerves. At the skin level, individual dermatomes from individual nerve branches can be under tension, so it is important to take them in the right direction and differentiate their distributions so as not to irritate a stretched nerve even further.
To help maintain length and proper ‘flossing’ of the posterior nerves, I recommend my clients do bodyweight- only squats and ‘good morning’ stretches with proper form and full range of motion. This keeps the posterior femoral cutaneous nerves, the sciatic nerves, and sural nerves nice and long. I encourage them to sit with their buttocks up and behind – not underneath – to keep the downward pull on the fascia to a minimum. In addition, the way pants, belts, and other clothing can pull on the superficial nerves can be an important source of the problem. If the pants ride low on the hips, the superficial nerves will be put under more chronic tension.
In the front, there are nerves that can also be part of idiopathic pain patterns that accompany back pain complaints and hip issues (see Figure 2). The lateral femoral cutaneous nerve originates at L2 and L3 and is part of the lumbar plexus. It passes behind the psoas and in front of the quadratus lumborus muscle, travels along the iliacus, passes under the inguinal ligament (where it can be trapped laterally near the ASIS, causing lateral-thigh parasthesia or pain), and then emerges through the fascia on the front of the leg, where several large branches fan out over the anterior lateral thigh and IT band. It is important to note that there is one branch (the gluteal branch), which tends to creep way around to the back of the leg, underneath the glutes, as part of the lateral rotational pattern of the fascia lata (see also Figure 1). Since other branches of L2 and L3 spinal nerves innervate the psoas, this neural strain pattern will be part of the shortening in the core.
This is the result of the tightening and twisting of the groin strap and the inguinal strap (or body retinacula) as described by Schultz and Feitis (1996). The groin strap is essentially a bunching and thickening of the superficial fascia at the crease of the hips. The anterior nerves, especially, can be caught in these creases. I suspect it results largely from prolonged sitting with slight external rotation to the fascia lata and other upper leg fascias. In fact, the rest of the fascia lata, as well as the deeper investing fascias of the quads, hamstrings, and adductors, will display this external rotational torsion. This means that every nerve crossing the hip is subject to torsion or twisting strain [Figure 2 (B)]. Sagging of the skin and superficial fascia adds more tension to the nerve sheaths all the way down the leg. The lateral femoral cutaneous nerve extends all the way down past the knee. This means that the downward pull along the fascia in the territory of that nerve ultimately can put tension on the L2 and L3 nerve roots and even, potentially, the spinal cord [Figure 1 (B)]. In a right innominate anterior tilt pattern, a stronger downward and lateral pull of the fascia and more pronounced tension and shortening on the anterior nerves of that hip will be part of the pattern. The torsional patterns will also include the femoral nerve, ilioinguinal nerve, the iliohypogastric nerve (anterior branch), and the obturator nerve (which innervates the adductors and skin over them. The lateral pull on the upper leg fascias toward the trochanter can make the skin along the inguinal area toward the crotch very thin.
The ilioinguinal nerve (Figure 2) can also be affected here. It passes directly through the psoas. Palpation along the tissue that rolls over the inguinal strap [Figure 2 (A)] will reveal these rolled and tethered nerves. The stretch of these nerves within the tissue rolls can be a source of sharp shooting pain when tethered small segments get acutely over- stretched during movement. In addition, the femoral nerve and obturator nerve will be affected by the lateral torsion of the fascia lata. In some people the obturator nerve, together with the adductors, is rolled severely anteriorly near the top of the thigh and posteriorly near the knee.
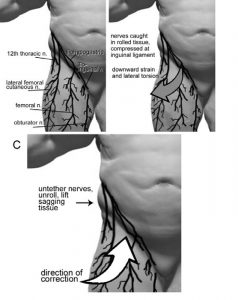
Figure 2: Anterior nerves involved in low back and hip issues. A – nerve anatomy adapted from Netter (1989). B – note how tissue can roll over the inguinal strap with nerves trapped at the crease. C – directions for repositioning fascia and nerves.
To relieve the strain here, I endeavor to reposition and de-rotate the entire fascia lata, working with the intention to feed the nerves and tissue back up and toward their origin or perforation site, as shown with the arrows in Figures 1 (C) and 2 (C). It is also important to restore glide locally and dampen any inflammation by gently pumping out the inflammatory fluid that contains nociceptive neurotransmitters and that can put turgor pressure on the nerve fibers. Alleviating strain on the lateral femoral cutaneous nerve and the other anterior nerves caught in the groin and inguinal straps can help considerably to tone the abdominals and reduce an overhanging belly, and help activate the psoas. A light gentle strumming motion to gently unroll the tissue headward at the inguinal strap is quite effective to free these nerves. Rolling of the IT band with foam rollers could be made more effective by attention to the direction of the lateral femoral cutaneous nerve. In this case, rolling to push the tissue upward with a vector as shown in Figure along the course of that nerve within the abdominal muscles to liberate it on that
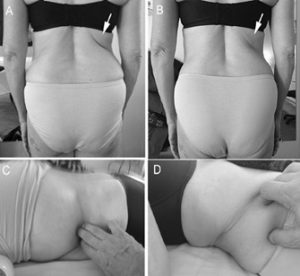
Figure 3: The twelfth thoracic nerve can help create compression at the waist. A – note the deep crease (arrow) that tracks exactly with the twelfth thoracic nerve before manipulation. B – note the diminished depth of the crease (arrow) after excavating the twelfth thoracic nerve from the tehters in the body wall, as shown in C (client prone) and D (client supine).
1 (C) helps to alleviate neural strain.
Rolling or stroking the tissue downward is less effective because it just stretches the lateral femoral cutaneous nerve even more. Flicking techniques with spiraling or lemniscate motion can also be used to liberate or potentially stimulate the most superficial nerve twigs. With self care, the direction of rolling with foam rollers is important and could be made more effective if the direction of neural strain is considered.
Posteriorly, the twelfth thoracic nerve (or subcostal nerve) emerges underneath T12 and travels through the body wall between the internal and external obliques and emerges to the cutaneous level just above the ASIS and the TFL muscle [Figure 1 (A)]. This nerve extends as far down as the TFL. Tethering over the TFL and tension along this nerve also helps to pull the rib cage down on the pelvis, shortening the waist and leaving less room for length in the lumbars.
An image of a client with a deep crease in her back along the course of the twelfth thoracic nerve is shown in Figure 3 (A). If you palpate carefully along such creases, you can track the nerves all the way down to their distal tether points. In or along the body wall, you’ll feel a bunching of the fascial tissue as it gathers around the nerve sheath. The tension along the nerve as it travels through the body wall and sagging of anterior tissues helps to create these creases. To address this, gently pick with fingernails and finger pads, detailing part of its pathway [Figure 3 (C and D)]. (Finger pads or gentle fingernails can be used along or around a nerve. Never crush a nerve with a fingernail.) Of course, you must also release its distal end, where it’s tethered over the TFL. If you palpate carefully, you will find there will be at least one tethered nerve at the base of any such telltale crease in someone’s back. After a bit of nitpicking along the course of the twelfth thoracic nerve, as shown in Figure 2 (C, D), the depth of the crease was reduced (B) and the client had a pronounced feeling of increased length through her core.
Some people require multiple sessions to reposition the tissue enough to alleviate the pull on all the nerves involved. It is important to note that tethering of the nerves all the way to the nail beds in the toes can foil our attempts to alleviate pain and restore function. Any nerve left tethered in the legs can help to pull someone back into his/her pattern. After effective de-rotation and lifting of the fascia containing the nerves, repositioning them higher on the leg, and removing the tension and torsional strain on the involved nerves, back pain will usually be relieved, and this helps to improve lift through the core and fluidity of movement around the hips and low back.
References
Stephen Evanko is a Certified Advanced Rolfer and conducts cell biology research at The Benaroya Research Institute in Seattle.
Barral, J.P., and A. Crobier 2005. Manual
Therapy for the Peripheral Nerves. Edinburgh: Churchill Livingstone Elsevier.
Evanko, S. 2010 June. “Getting a Handle on the Superficial Fascia – In Consideration of the Cutaneous Nerves.” Structural Integration: The Journal of the Rolf Institute® 38(1):12–15.
Maigne, J.Y., J.P. Lazareth, H. Guérin Surville, R. Maigne 1989. “The Lateral Cutaneous Branches of the Dorsal Rami of the Thoraco-lumbar Junction.” An Anatomical Study on 37 Dissections. Surgical and Radiologic Anatomy 11:289– 293.
Maigne, J.Y., R. Maigne 1991. “Trigger Point of the Posterior Iliac Crest: Painful Iliolumbar Ligament Insertion or Cutaneous Dorsal Ramus Pain? An Anatomic Study.” Archives of Physical Medicine and Rehabilitation 72:734–737.
Netter, F.H. 1989. Atlas of Human Anatomy. S. Colacino, ed. Summit, New Jersey: Ciba-Geigy Corporation.
Sauer, S.K., G.M. Bove, B. Averbeck,
P.W. Reeh 1999. “Rat Peripheral Nerve Components Release Calcitonin Gene- related Peptide and Prostaglandin E2 in Response to Noxious Stimuli: Evidence That Nervi Nervorum Are Nociceptors.” Neuroscience 92:319–325.
Schultz, L. and R. Feitis 1996. The Endless Web: Fascial Anatomy and Physical Reality. Berkeley, CA: North Atlantic Books.
Wilke J., R. Schleip, W. Klingler, C. Stecco 2017. “The Lumbodorsal Fascia as a Potential Source of Low Back Pain: A Narrative Review.” BioMed Research International Epub 2017 May 11.
2017;2017:5349620