
Objectives: The objectives of this report are to review the clinical practice of Structural Integration (SI), an alternative method of soft-tissue manipulation and sensorimotor education, and to summarize the evidence to date for mechanism and clinical efficacy.
Methods: The author’s personal knowledge of SI literature, theory, and practice was supplemented by a data- base search, consultation with other senior SI practitioners, and examination of published bibliographies and websites that archive SI literature.
Results: SI purports to improve biomechanical functioning as a whole by progressively approximating specific ideals of posture and movement, rather than to treat particular symptoms. Hypothesized mechanisms at the level of local tissue change include increases in soft-tissue pliability, release of adhesions between adjacent soft- tissue structures, and increased interstitial fluid flow with consequently improved clearance of nociceptive potentiators. Hypothesized mechanisms for more global changes include improved biomechanical organization leading to reductions in mechanical stress and nociceptive irritation, a perception of improved biomechanical efficiency and coordination that generalizes to the self, and improvements in sensory processing and vagal tone. Emotional catharsis is also thought to contribute to psychologic changes. Limited preliminary evidence exists for improvements in neuromotor coordination, sensory processing, self-concept and vagal tone, and for reductions in state anxiety. Preliminary, small sample clinical studies with cerebral palsy, chronic musculoskeletal pain, impaired balance, and chronic fatigue syndrome have reported improvements in gait, pain and range-of-motion, impaired balance, functional status, and well-being. Adverse events are thought to be mild and transient, although survey data are not available. Contraindications are thought to be the same as for massage.
Conclusions: Evidence for clinical effectiveness and hypothesized mechanisms is severely limited by small sample sizes and absence of control arms. In view of the rapidly increasing availability of SI and its use for treatment of musculoskeletal pain and dysfunction, more adequate research in warranted.
Introduction
Structural Integration (SI) is a system of manual therapy and sensorimotor education that aims to improve human biomechanical functioning as a whole rather than to treat particular symptoms. It was developed and propagated by the biochemist Ida Pauline Rolf (1896–1979) in the midand late 20th century. The past decade has seen a rapid in- crease in the number of practitioners and training institutions, both within the United States and internationally. SI techniques have been adopted by a wide range of other manual therapies, and the method is increasingly resorted to for the treatment of chronic musculoskeletal pain and dysfunction (1). Of the many prior accounts of SI, the few that discuss research on its effects or mechanisms do so in a narrative mode, omit important details, and do not comment on methodological quality (2–6). Those limitations and the publication of more recent studies warrant an updated, more systematic review.
The summary of theory and clinical practice that is presented here is drawn from the author’s training with Rolf in 1972–1974, his experience as an SI practitioner, and his familiarity with the literature. These were supplemented by discussions with other senior SI practitioners. Candidates for review were identified by searches of PubMed (on structural integration and Rolfing®*), examination of published bibliographies, and from websites that archive SI literature.7–9 Six (6) mechanistic studies10–15 and six clinical studies16–21 all reporting quantitative outcomes and with sample sizes greater than five were included. Eight (8) case study reports with fewer than 5 subjects each were excluded because of their negligible evidentiary value.22–29
Theory
Rolf regarded gravity as a major, lifelong stressor to which all human beings must adapt, and believed that the efficiency of movement or distress inherent in various patterns of adaptation is of great significance for the individual’s health and quality of life.30–34 She developed postural and movement ideals to serve as hallmarks of optimal adaptation to gravity (i.e., minimal stress and maximal efficiency). The most prominent of these are alignment of the major body segments—cranium, thorax, pelvis, knees, and feet—in relaxed standing such that the center of mass of each falls along the ‘‘gravity line,’’ the vector of gravitational force that defines vertically. Other guiding ideals are bilateral symmetry, and anterior–posterior ‘‘horizontality’’ of the pelvis, thorax, and cranium. Movement ideals include a uniformity of tonus that allows all activated muscle groups to contribute equally to the work of movement (Rolf called this ‘‘grace’’), and efficient neuromotor coordination in everyday activities, often assessed by the extent of cross-extensor activation in walking (counter-rotation of pelvic and shoulder girdles). The goal of SI treatment is to progressively approximate the individual’s structure and movement to these ideals. Rolf also believed that her method would increase the individual’s integration with the Earth’s gravitational field, that this would promote ‘‘greater psychological ease and emotional security,’’ and that the ‘‘integrated man’’ would manifest increased ‘‘maturity.’’ She regarded the alleviation of chronic musculoskeletal or other conditions as byproducts of progress toward these more holistic goals.35
Clinical Practice
The methods of SI are both manipulative and educational. Manual force is applied to the soft tissues in a manner that is generally more gradual and prolonged than is typical of chiropractic or osteopathic manipulation, yet with more pressure than is typical of massage. The client most often lies on a cushioned treatment table, but may also be seated or standing. The practitioner makes contact with fingertips, knuckles, a closed fist or the flat of the ulna, sustaining pressure until the tissue is felt to ‘‘give,’’ which is taken as an indication that its pliability has increased. In order to in- crease the area over which soft tissue change occurs, the client is often asked to perform slow, directed movements as pressure is applied.
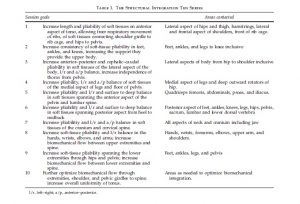
Rolf formulated a series of 10 treatments, referred to as ‘‘the Ten Series,’’ as an initial course of therapy (Table 1). Each lasts approximately 1 hour and focuses on a specific set of biomechanical changes that are intended to advance the overarching ideals. In addition to the particular goals of each session, each also concludes with work that provides additional flexibility to the spine so that vertebrae can realign in Rolf also devised postural and movement awareness exercises that contribute to the goals of each of the Ten Series sessions. The client is asked to perform specific, simple movements while directing attention to ‘‘landmark’’ points on the body. These directions are often enhanced by imagery. The exercises are designed to cultivate the ability to dis- criminate between established habits that entail more versus new patterns that entail less biomechanical strain. They may be supplemented by sessions of Rolf Patterning, a system of movement awareness training that was developed to complement SI treatment.
Contraindications are thought to be the same as for mas- sage. Adverse outcomes are anecdotally rare when treatments are delivered by a practitioner trained at the Rolf Institute or a school of comparable quality. Kerr reports a single instance of an adverse outcome: the displacement of a urethral shunt,39 and adverse events are also noted in one small clinical study,16 but survey data have not been re- ported. The most typical dysphoric concomitants are transient soft-tissue pain during the actual manipulation, rarely bruising at the site of contact, and transient increases in anxiety or other negative affect that resolve spontaneously within a few hours or days. Following the resolution of the latter, clients often report reduced levels of anxiety or depression, and that those improvements persist longterm.35,40,41 response to the changes induced in other areas* (Table 2).

*The goals of each of Rolf’s 10 sessions and those of several de- rivative systems of SI have been detailed in a series of articles by Tom Myers.1,36,37 Deutsch and James also give brief descriptions of the 10 sessions.18,21
Purported Effects, Hypothesized Mechanisms, and Mechanistic Studies
Increased soft-tissue pliability and independence of movement*
The most commonly reported local effects are increased pliability of the soft tissues and increased independence of movement between adjacent soft tissue structures; the latter conceptualized as the release of ‘‘adhesions.’’ It is also commonly reported that sustained manual pressure at one lo- cation may increase soft-tissue pliability over a wider contiguous area (i.e., the local change seems to ‘‘spread’’). Rolf believed that these effects were due to changes in the biomechanical properties of the soft connective tissues. Myofascial sheets are, in fact, continuous over areas much larger than the individual muscles they ensheath.45,46
Rolf also suggested two other consequences of local in- creases in what she believed to be fascial pliability. The first is an increased rate of interstitial fluid flow, which is potentially significant because movement through the soft tis- sues accounts for a large portion of fluid transfer in the body. The second is that the increased pliability and movement of the myofascial sheets increased the stimulation of sensory nerves and thus enhanced somatosensory perception.
None of these hypotheses about the local effects of SI manipulation have been quantitatively assessed.
In developing Patterning, Rolf collaborated with the dance teacher Judith Aston, who later broke away to teach her own system of manipulation and body awareness.38
In addition to the hypotheses reviewed here, less formalized rhetorics of ‘‘balancing’’ or ‘‘refining energy’’ are also common in the SI community. Oschman has provided the most comprehensive re- views of their scientific plausibility.42–44
Reductions in pain
Rolf taught practitioners to approach joint pain and dysfunction by comparing the tone and motility of all the soft-tissue structures that are called upon to lengthen and contract as the joint flexes and extends. Pressure is then applied to structures that are visibly less motile than others, resulting in a subsequent increase in their ability to flex and extend. Clients often report that the entire area—both the joint and surrounding tissues—subsequently feels less painful, ‘‘better,’’ and ‘‘stronger.’’ Rolf regarded this effect as due to a reduction in mechanical strain resulting from improved tone in the involved soft tissues; that greater equality of tone allows strain to be shared more equally among all involved soft-tissue structures, rather than the few that are more capable of stretch being required to bear excessive strain. However, neither this hypothesis, nor its association with improvements in joint pain and function, has been quantitatively studied.
Rolf appears not to have posited a more general mechanism for a widely reported reduction in chronic musculo- skeletal pain. However, Deutsch et al., in a review of clinical records that found significant benefits for a variety of chronic musculoskeletal pain syndromes, discusses three ways that SI might reduce nociceptive stimulation.18 They first extend Rolf’s thesis that balancing the pliability of connective tissues in the area of problematic joints can realign force vectors along more physiologic lines by noting that this might also reduce nerve irritation at the joint. Second, they note that SI is often reported to increase the flexibility of scar tissue, the rigidity of which is theorized to be another source of nociceptive irritation. Finally Deutsch et al. suggest that the increased rate of interstitial fluid flow that Rolf believed SI produced might relieve local ischemia due to an impaired perfusion that would contribute to local hypoxia, acidosis, and the accumulation of bradykinins, potassium ions, and prostaglandins, all of which are known nociceptive amplifiers.47 However, none of these hypotheses has been quantitatively investigated Improvements in overall posture and movement
The most commonly reported whole-body effects are improvements in posture and motor coordination, and in- creased overall relaxation. These are often reported immediately following a treatment, but longer-term onset is also noted. Rolf attributed these to the migration of the client’s structure and movement patterns toward increased biomechanical efficiency in response to strategic changes in the pliability of the soft tissues and increased somatic awareness. A number of publications have provided photo- graphic documentation of dramatic improvements in standing posture, but no quantitative assessment has appeared.31,32,34,40,48 These changes in posture and movement could be the result of alterations in muscle tone as well, but neither Rolf’s hypothesis nor that of change in muscle tone have been quantitatively investigated.
In an electromyographic study of the performance of 11 healthy males on a panel of standardized motor tasks pre- versus post-10 SI treatments, Hunt found increases in the rhythmic coherence of motor neuron activation, functional independence of muscles, efficiency of movement, and improved posture12 (Table 3, row 1).


Psychologic benefits
Anecdotally reported psychologic effects include in- creased self-confidence, more proactive and less reactive behavior, increased tolerance for emotional experience, in- creased stability under emotional stress, and reductions in anxiety and depression.35,40 Rolf attributed these in part to a generalization of the client’s experience of improved bio- mechanical stability and coordination to the affective and social aspects of the self. However, the association between biomechanical improvement and psychologic benefits has not been quantitatively evaluated.
She also regarded chronic rigidities of the myofascia as capable of storing negative emotional memories, and that these could be released following the increase in soft-tissue pliability produced by SI manipulation, much in the manner theorized by Wilhelm Reich.49 However, the association be- tween increased soft-tissue pliability, emotional catharsis, and subsequent psychologic benefit has not been quantitatively investigated.
Two (2) studies have found psychologic improvement to be associated with SI treatment. In a group of 24 SI clients, Pratt found significantly more positive averages pre- versus post- the 10 sessions on two items of the Semantic Differential–My Psychological Self and Cheerful11,50 (Table 3, row 2). Weinberg found a significant reduction in state anxiety in 24 healthy adults pre- versus post-10 sessions of SI, an effect not found in a control group of equal size given 10 sessions of exercise13,51 (Table 3, row 3).
Neurophysiologic mechanisms
Although Rolf did not discuss the possible neurophysio- logic effects of SI, several hypothesized mechanisms of that type have been investigated.
Silverman proposed that SI improved sensory processing in ways that would contribute to psychologic health. In a sample of 13 healthy adults, he found significant pre- versus post-treatment changes in three parameters derived from electroencephalographic data. These were interpreted as in- dicating a more receptive orientation to sensory stimuli, in- creased capacity for the efficient organization of sensory input, and a shift from an ‘‘augmenting’’ to a ‘‘reducing’’ style of adaptation to differences in stimulus intensity10 (Table 3, row 4).
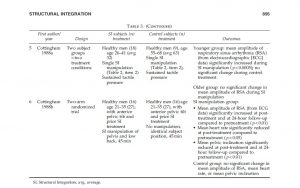
Cottingham reported a transient but statistically signifi- cant increase in the mean amplitude of respiratory sinus arrhythmia (RSA), interpreted as an index of vagal tone,52 in a group of 18 young adult to middle-aged men during a single manipulation of the sacrum and lower lumbar area. This was the ‘‘pelvic lift,’’ which is a key element of Rolf’s treatment protocol (Table 2, item 2). That effect was not significant when the same group underwent a tactile stim- ulation control, nor when a group of 9 older men was treated with pelvic lift14 (Table 3, row 5). A follow-up study found a significant increase in mean amplitude of RSA and a de- crease in sagittal pelvic tilt pre- versus post-45 minutes of SI manipulation of the pelvic region in 16 healthy adult men who had previously undergone 10 sessions of SI. Both effects were maintained at 24-hour follow-up. Neither occurred in a comparison group of the same size who were matched for age and prior SI treatment and who received a time and postural position control15 (Table 3, row 6).
Clinical Studies
Cerebral palsy
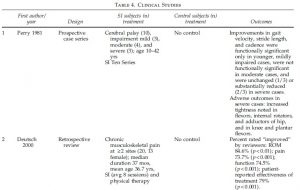
Perry et al. studied biomechanical changes in a series of 10 patients with cerebral palsy pre- versus post- the SI Ten Series. They found that improvements in gait velocity, stride length, and cadence were functionally significant only in younger, mildly impaired cases, less pronounced and not functionally significant in moderate, and absent in severely impaired cases. Immediately following the Ten Series, some of the latter group showed increased impairment of stride and increased muscle tightness in the lower extremities. These were interpreted as contraindicating SI for severe cases16 (Table 4, row 1).
Chronic musculoskeletal pain
Deutsch reviewed the clinical records of 20 patients who were treated with SI for chronic musculoskeletal pain in a rehabilitation clinic. Each patient had pain at two or more sites. Conditions included trochanteric and subacromial bursitis, low back and cervical pain, sciatica, and general myofascial pain syndrome. The reviewers rated significant percentages of cases ‘‘improved’’ in range of motion (ROM), and in patient-reported pain, functional status, and well- being. However, 70% of the sample had received physical therapy concurrently, making it impossible to attribute the outcomes unambiguously to SI18 (Table 4, row 2).
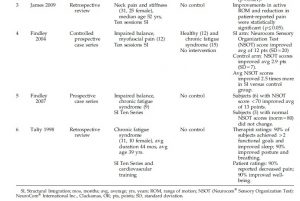
More recently, James et al. reviewed the clinical records of 31 patients who were treated with 10 sessions of SI for neck pain and stiffness in a physical therapy practice. They found significant average improvements in active ROM and patient-rated pain21 (Table 4, row 3).
Impaired balance
Findley used the NeuroCom® Sensory Organization Test (NSOT) (NeuroCom International Inc., Clackamas, OR) to measure standing balance in 12 patients with myofascial pain pre- versus post- the SI Ten Series. Balance scores improved 2.5 times more in this group than in an untreated control group composed of 12 healthy and 16 subjects with chronic fatigue19 (Table 4, row 4). In a follow-up study, Findley et al. reported on changes in NSOT scores of 9 patients with chronic fatigue pre- versus post- the Ten Series. Six (6) who had initial balance scores below 70 improved an average of 13 points (a score of 80 is considered normal), and the scores of 3 subjects with normal balance did not change20 (Table 4, row 5).
Chronic fatigue syndrome
Talty et al. reported on 11 cases of chronic fatigue syndrome treated with SI and a cardiovascular endurance regimen. Improvements were noted in therapist ratings for sleep, posture, breathing, and achievement of functional goals, and in patient ratings of pain and well-being17 (Table 4, row 6).
Conclusions
Of the therapeutic mechanisms that have been hypothe- sized, preliminary evidence is suggestive for improvements in neuromotor organization,12 sensory processing,10 and self- concept,11 reductions in state anxiety,13 and increased vagal tone.14,15 Preliminary clinical studies with small samples of patients with cerebral palsy, chronic musculoskeletal pain, impaired balance, and chronic fatigue syndrome suggest positive effects on gait,16 musculoskeletal pain and associ- ated ROM limitations,18,21 impaired balance,19,20 and func- tional status and well-being.17,18 Adverse outcomes are reported in a single case39 and one small case series.16 The evidence for clinical effectiveness and mechanisms alike is severely limited by small samples sizes and the absence of placebo or other comparison control arms in most studies. In particular, the contribution of placebo effects to reductions in pain and to psychologic benefits may be significant and should be investigated. Given the rapid increase in the availability of SI and its use for the treatment of chronic musculoskeletal pain and dysfunction, better-designed, controlled studies with adequate sample sizes are desirable.
Acknowledgments
Assistance in identifying relevant literature and obtaining research reports was provided by Tom Findley, Rosemary Feitis, Aline Newton, and Valerie Berg, all members of the Rolf Institute of Structural Integration. Guidance in manuscript preparation was provided by Ted Kaptchuk of the Osher Research Center, Harvard Medical School, Helene Langevin of the University of Vermont School of Medicine, and Rosemary Feitis. Research and manuscript preparation were supported by grants K01AT004916 and K24AT004095 from the National Center for Complementary and Alter- native Medicine, National Institutes of Health.
Disclosure Statement
The author is a practitioner of Structural Integration, chairperson of the research committee of the Rolf Institute of Structural Integration, and a member of the scientific review committee of the Ida P. Rolf Research Foundation.
References
Structural Integration, an Alternative Method of Manual Therapy and Sensorimotor Education[:]