
Introducing Foot Maps
To evaluate the effects of the Rolfing® Structural Integration (SI) process, we normally use the client’s sensation in relation to particular complaints; still photographs or videos of the client in motion; and the client’s subjective reports. This article presents another instrument of evaluation – the foot map – that may be used throughout a series to track the client’s relationship with gravity in standing and walking.
The foot map also demonstrates the importance of the oral functions to the gravity relationship. After having practiced SI for twenty years, I directed my attention to the science of speech therapy to gain a better understanding of the powerful connection between the mouth and the feet. This connection has a clear evolutionary basis, as the locomotor system developed to facilitate the pursuit and capture of food. I also undertook a program of postgraduate study in psychomotricity, which is the study of the relationship of physical movement to cognitive, affective, and psychosocial behaviors.
As a means of therapeutic evaluation, the foot map serves the following functions:
Making the map is simple, and begins with asking the client to notice in standing which parts of the feet support the weight, and in walking which parts receive weight and which push off. Next, the client stands on a piece of paper while the practitioner draws an outline around each foot. Then the client draws onto the outlines a representation of his or her felt sense of which parts of the feet are active for support, receipt of weight, and propulsion. To facilitate use of the maps to track changes over time, it is helpful to have pencils or pens of various colors. (As this journal’s images are in black and white, the foot maps show in this article will incorporate bold, crosshatching, and other means to show changes over time.)
For the client, the experience of sensing and drawing the areas of the feet that make contact with the ground, both at rest and in walking, generates a symbolization of the client’s relationship with gravity. To observe from the outside the representation of what s/he is feeling from the inside can offer the client valuable insights as to how the s/he is organized in gravity; and how the client uses the map can be an additional reference point for recognizing changes. For the practitioner as well, the foot maps gather various data points about the client’s organization:
INTERVENTIONS
The Second Hour of a Ten Series is an ideal time to introduce the foot map. I generally ask the client to map his/her feet before and after the session to reveal which parts of the feet make contact with the ground in standing and walking, and what changes came about from the session.
In the Third Hour, when our concern is with the lateral line, I suggest to the client another experience — to bite down evenly and methodically on a length of rubber surgical tubing. 1) This ameliorates the
distribution of weight over the feet because the muscles of mastication are intrinsically connected to stress-driven heightening of muscular tonus generally. The powerful flexors of the mandible effect an antigravity action throughout the entire body through the lateral line. 2) The action of chewing, as it passes through the phases of working side and balancing side, neutralizes excessive tonus in the muscles of mastication and brings better support to the cuboid and the entire lateral aspect of the foot — including the fourth and fifth toes, which, according to Tom Myers, stabilize the body weight. (The muscle chain of the lateral line is described in his Anatomy Trains materials.) In my own practice, I often notice that clients have lost the support of the lateral toes, which compromises the weight stabilization that must start in the feet and ankles. This compromise, in turn, transfers the task of supporting the body weight to other more proximal joints, which then become overloaded, and subject to strain, excess wear and tear, and lesions. See Figure 5 and commentary.
Often, the antigravity muscles exert more force on one side than on the other, which can produce various lateral asymmetries, e.g., differences in the height of the shoulders or iliac crests or between the malleoli, as well as inclinations of the head. Following manipulations to address these lateral asymmetries, we are likely to observe greater symmetry and balance in the distribution of weight over the feet. I also use specific chewing exercises to address lateral asymmetries: since the muscles of mastication are key to the antigravity response, balancing the tonus of these muscles tends to carry through to other antigravity muscles. See Figures 6 through 9 and commentary. [My earlier article (Pacheco 2010) discusses the oral reflex functions and the benefits of exercises to improve them.]
The Fourth-Hour work equilibrates the tonusoftheentiremuscularchainthatbegins with the hallux and runs through the medial line of the leg, iliopsoas, diaphragmatic crura, transverse musculature of the thorax, and the infrahyoid muscles and hyoglossus (which originates in the tongue), which insert to the hyoid bone. Here, I often suggest to the client another oral exercise that acts on the entire medial line, with the goal of increasing the propulsive force of the feet through better use of the psoas. These are exercises to coordinate and strengthen the internal and external musculature of the tongue and lips. They are rhythmic and are executed with tonic musculature, which brings connection and good tone to the deep medial line. See Figures 7 and 10.
As a direct intervention with the feet, I also use exercises for differentiation and integration of various structures. For example, I ask the client to stand with one foot on a slender stick (about one-half inch in diameter), which I place lengthwise under either successive metatarsal interspaces or successive metatarsal bones (see Figure 1), starting at the lateral foot and working medial. The client is asked to raise the opposite foot; flex and extend the knee on the supported foot; and then return the opposite foot to the ground. The sequence is repeated three times for each placement of the stick. This helps to differentiate the rays of the toes, and also to create space between them.
Another exercise that helps the client to differentiate and activate the metatarsal interosseus muscles is to place a pen or pencil between the seated client’s toes and ask the client to discard the object with movement of the toes only.
Along with these exercises — especially for clients with diminished arches — I

Figure 1: Stick placed under third metatarsal.
like to add another one to differentiate and strengthen the interossei. With legs extended, the seated client is given an elastic band to wrap around one toe at a time (see Figure 2). The client tugs on the band to apply tension to the toe, and then plantar- flexes the toe, against resistance from the band, at the metatarso-phalangeal joint.

Figure 2: Plantar flexion at the metatarsophalangeal joint, resisted with elastic band.
Case Study Discussions
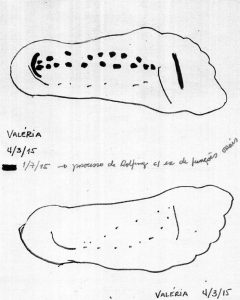
Figure 3
Figures 3-10 will be used for brief case studies to show the maps in use. Each map includes various temporal elements, drawn with different lines, as discussed below.
In Figure 3, Valeria’s complaint was pain in the left shoulder. On the initial map (the fine lines in the drawing), we can see how the lateral aspect of the left foot is suspended. This caused me to hypothesize that the painful shoulder was holding the weight of the body out of the left foot; and this hypothesis helped me to organize the Rolfing series. The area in bold was drawn after manipulation along with oral- function exercises. Even after our work was complete, the dotted lines on Valeria’s maps suggest that she senses only weakly her body weight arriving to the ground.
Sandro (Figure 4) is a runner, and presented with complaints of body pain in many locations. On Sandro’s map, the areas drawn lightly were the ones he identified initially, and from those it appeared that he was tilting over to the right side, with more weight in the right lateral foot and stronger push-off through the right foot than through the left. Foot exercises – to open the interosseus spaces of the foot, lengthen the lateral and posterior muscle chains, and mobilize the ankles – improved Sandro’s functional balance in both standing and walking: he drew the bold lines on the map after that process. Observe also that Sandro’s map reflects a better sense of his own body weight than Valeria’s (Figure 3).
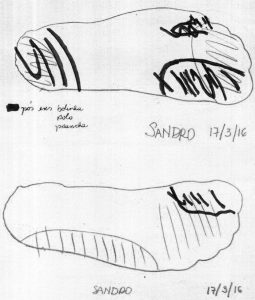
Figure 4
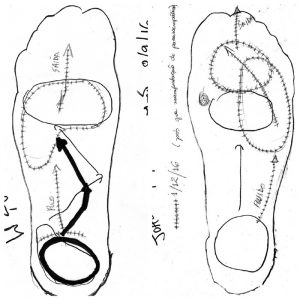
Figure 5
João’s complaint was pain in the left temporomandibular joint (TMJ). The oral exercises released tension that had been suspending the left lateral line and throwing the arch of the foot medially in walking (Figure 5). In João’s case, after the lateral line was released, he gained greater support from the lateral foot. This, in turn, amplified his push-off and brought the left transverse arch more lateral. At the same time, his sensation of pain in the left TMJ diminished. Observe also how a shift in the balance of the autonomic nervous system was followed by greater symmetry in João’s felt sense of his two feet. The bold area was drawn after mastication exercises; the crosshatched areas came into awareness following a parasympathetic surge that included vomiting and diarrhea.
Rodrigo (Figure 6) complained of multiple pains in his back. Both iterations of drawings on Rodrigo’s map were made on the same day — during the Third Hour, but before and after he performed mastication exercises. This technique helps the practitioner to evaluate the degree to which the muscles of mastication are involved in the client’s postural pattern. The areas in fine lines were those identified at the outset, when we could see both that Rodrigo’s axis was inclined to the right, and that his weight was distributed over his right foot. The bold lines drawn after the mastication exercises show that the lateral aspect of the left foot could then take support from the ground, which allowed Rodrigo’s weight to be more evenly distributed over both feet.
Karol (Figure 7) complained of great pain in her neck, particularly on the right side. Observe from the light lines that before Karol performed the mastication exercises, there was no place on the right foot for her weight to arrive, nor was there any possibility of shock absorption on that side; moreover, it looked as if the right foot was suspended through the medial line. In this Fourth Hour, the left medial line was addressed only lightly. After manipulation of the right medial line followed by mastication exercises, the bold areas indicate that her foot found someplace to receive her weight, as well as greater medial support (which indicates more functional arches). By the end of the session, she no longer felt pain in her neck and did not complain of neck pain thereafter.
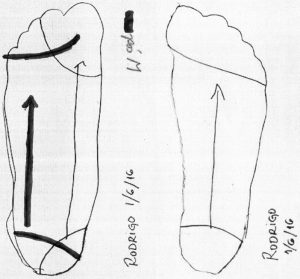
Figure 6
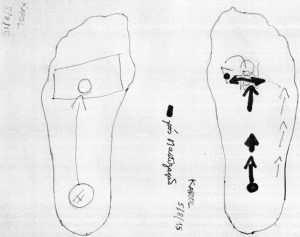
Figure 7
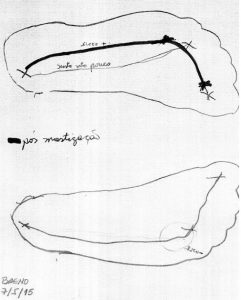
Figure 8
Breno complained of pain in his right hip and presented with his axis inclined to the right. In his initial drawing, indicated in the lighter lines in Figure 8, he sensed only weakly: the line on the left foot connecting the heel to the metatarsal heads and toes was drawn to suggest weak sensation, allowing his weight to fall more over the right foot, and making his weight shift over to the right side. There was a great deal of tension on the right in his rotators, psoas, and quadratus lumborum, while on the left side, his lateral line was suspended by the muscles of mastication. Breno benefitted from the mastication exercises, and shortly after he had practiced them, he drew the new points of contact that he perceived (bold lines) as he sensed more strongly. Throughout the process, his hip pain returned from time to time; at those times, he would show me on the foot map the places where he had lost support. The map was very important to Breno’s process because it kept him hopeful that he would be able to relieve his pain through organizing his understanding of the relationship of his center to the ground.
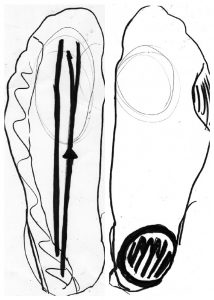
Mauricio (Figure 9) presented with low back pain. Based on his initial foot map (fine lines), it appeared that a pelvic rotation had thrown his weight to the lateral left foot. This rotation was barely visible when Mauricio was standing, though he presented with a straightened lumbar lordosis and his pelvis tilted anterior. There was a compensation: his right leg and foot were abducted out into an open diagonal, such that on the right he used only a small portion of the forefoot both to receive his body weight and to propel it forward. The mastication exercises brought him additional areas of support (bold lines), while the Fourth Hour (effect drawn in circles) was key in letting his midline access support over the feet. Because the map was a visible, external representation of Mauricio’s subjective sensations, it allowed him to communicate those sensations. It also brought him the ability to perceive the support available to him, and also to visualize those areas of the foot he was not using. Finally, he was able to relate the improved support to the absence of low back pain. He found the process to be enormously valuable.
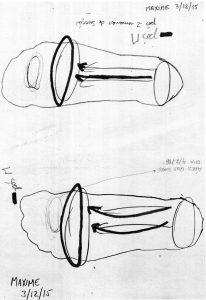
Maxime arrived on the advice of his psychotherapist, who was treating him for depression. For Maxime, the foot map (Figure 10) – which brought his attention to the use of his feet – was an important reference throughout his process. Following the mastication exercises, when he added the bold lines to the map, he perceived that there was a large area of his feet that he had not been using, and he connected this to his lack of propulsion in life. The map helped direct his attention and action toward occupying previously unused areas of his feet, including the metatarsals and toes. He found the proprioception-based graphic representation of his situation to be an organizing mechanism for him to understand the process as a whole. During the time we were working together, he climbed a mountain and began bicycling, and regularly performed exercises for the oral functions of both mastication and sucking. Gradually, he recovered the ability to move forward – both in walking and in his life.
Conclusion
Mapping the feet brings different improvements in sensation and perception to different clients. Sometimes the maps bring improved sensation at a particular point in the process, while for other clients the maps help to orient the process as a whole. But for me as a Rolfer, the maps reveal treasures for the Rolfing process every time.
Beatriz Pacheco is a Certified Advanced Rolfer, Rolf Movement practitioner, speech therapist, and psychomotrician with a practice in São Paulo, Brazil.
Bibliography
Pacheco, B. 2010 Jun. “Including Functional Exercises in the Seventh Hour.” Structural Integration: The Journal of The Rolf Institute® 38(1):36-40.
Maps of the Feet[:]