Introduction
In most health-care disciplines, the best idea is to not treat pain complaints without a clear and accurate assessment of the problem. The easiest way to arrive at an accurate assessment is after a complete case history has been taken and reviewed and after a thorough physical examination has been rendered. In any type of pain management, if this explicit process is followed, the risk to the client’s welfare is minimized.
Neurological entrapment symptoms are due to nerve damage as a result of chronic mechanical compression. Most neurological entrapments are classified as syndromes. It is common for this compression to occur in the body’s more narrow passages or in tissues that have been compromised in some way. It is a biomechanical issue and not an issue of pathology.
Taber’s Cyclopedic Medical DictIonary(1) defines a “syndrome” as a group of symptoms, signs, laboratory findings and physiological disturbancs that are linked by a common anatomical, biochemical, or pathological history. Syndromes that Rolfers most often hear about in their treatment rooms include carpal tunnel syndrome (CTS), performs syndrome, and perhaps thoracic outlet syndrome. Less frequent diagnoses include dorsal scapular entrapment, long thoracic entrapment, and pronator syndrome.
The primary purpose of this paper is to present the clinical features of some of the more common mechanically induced neuropathies. This paper is not meant to be construed as a treatment guide or a substitute for appropriate examination and/or care. It is very important to recognize the gross signs of a systemic disease that mimics neuromusculoskeletal problems and to be in a professional position to refer out to the appropriate physician promptly.
The “red flags” of low back/lower extermity pain are: bilateral ridiculer pain, ridiculer pain below the knee, a failed “toe walk” test, a failed “heel walk” test, and inability to control the bowels/bladder. These conditions are, for the vast majority of cases, strong indications for an immediate allopathic referral.
There are four basic types of pain. Neuropathic pain is the direct stimulation of pain-sensitive neurons where the pain is worse at night. Muscular pain is worse during the day when activity is increased. Inflammatory pain is worse first thing in the morning and during activity. Lastly, mechanical pain increases during activity and often eases at night with lying in bed in a certain position.(2)
Early on, you need to determine whether the client is in the appropriate office, or needs other medical care. General early screening questions while reviewing the client’s case history include: “Where is your pain?” Is the pain easily pinpointed or is it a diffuse pain over an area? Does it travel or extend from one place to another? We want to know whether the complaint is focal or ridiculer. In general, focal pain issues are biomechanical in nature, and ridiculer pain follows a [nerve] pathway in the body. Keep in mind, though, that biomechanical pressure on a nerve can cause ridiculer symptoms.
A general physical examination technique for “Tinel’s sign” is often helpful in assessing the subjective complaint. A compromised nerve becomes sensitive to mechanical forces such as tapping, so you tap along the path of a peripheral nerve, proximal to distal from the suspected entrapment site. If it reproduces the client’s complaint of paresthesia and other sensor complaints, this is a positive on the test for Tinel’s sign.(3)
Understanding these fine points will help the practitioner make an appropriate and accurate assessment. From the ideas put forth here, it becomes apparent that the assessment of a neruological entrapment condition is one of exclusion: a process of ruling out factors in the case.
There needs to be a working understanding of the difference between ridiculer issues and issues of contractures. For example, some practitioners mistake a complaint of pain running down the back of the leg, from the client’s buttock to heel, as sciatic pain, but the sciatic nerve only runs down the back of the leg to the knee – from there it travels around the lower leg. The client’s issue may instead be a mechanical condition of myofascial contracture of the extensors. Continued questioning during the case review and physical examination, with one focus being on client’s exercise routines, may reveal more clues for a more accurate assessment.
Neruological entrapment more often than not refers to an area or region of localized injury to a peripheral nerve. Exogenic or endogenous trauma occuring at an entrapment point causes biomechanical irritation and initiates an inflammatory response; repetitive motion exacerbates this.(4) The injury may be directly to a nerve trunk or to the intrinsic blood supply of that trunk. The results include swelling of the nerve trunk, degenerative tissue change, and finally fibrotic tissue replaces normal tissue that has been injured. With both time and repetitive movement, symptoms become more apparent.
Peripheral nerves have to be able to move freely in relation to their surrounding tissues. Blood vessels have the necessary inherant elasticity to stretch, say when an extremity is moved. Nerves must be free from their dorsal roots to termination points to slide within surrounding tissues. When this movement is restricted, you have a case of neurological entrapment.(5)
There are three types of neruological entrapment: sensory, motor, and mixed. A prominent feature of sensory neruological entrapment is pain related to the nerve’s distribution area. This pain may be perceived as sharp, burning, or any number of other related perceptions. Other sensory experiences can include paresthesia and skin texture changes. Nerves where we commonly see sensory-based neurological entrapments include the lateral femoral cutaneous nerve, the saphenous nerve, and interdigital nerves.(6)
Motor neurological entrapment pain is not as well localized or definable. It covers a wider area, and over time the affected musculature atrophies. Examples of nerves where this type of neurological entrapment can occur are the deep branch of ulnar nerve, the personal nerve, and the ilioinguinal nerve.
The mixed entrapment pattern presents a combination of vascular and motor nerve symptoms. Examples of mixed nerves that can be affected in entrapments are the ulnar nerve at the elbow, the personal nerve in the lower leg, and the ilioinguinal nerve in the pelvis.(7)
The common features found in neurological entrapment are as follows. The client will report pain at rest as opposed to pain during movement. Often, this pain will be reported as worse at night than during the day. (We become more aware of these feelings because we have less stimulus input at rest or before sleep.) Passive or active movement of the affected area may exacerbate his/her complaint. “Valleix’s phenomenon” may be observed here: that is, both proximal as well as distal points along the nerve path may be reported as tender or painful. An example of this condition is in interdigital neuroma causing pain that travels up the sciatic nerve trunk into the lumbar region of the spine. Observation of this event is common in neruological entrapment syndromes where there are multiple insults along a nerve path. Chiropractic and scant allopathic literature citations list this occurance as the “double crush syndrome” where the proximal component of a nerve is injured, which predisposes the same nerve to a greater risk from a distal insult. For example, a patient with, say, a lower cervical radiculopathy may be more susceptible to a subsequent median or ulnar nerve injury.(8)
Here is a bit of an epidemiological perspective of various neruological entrapments: carpal tunnel syndrome is four times more prevalent than ulnar nerve entrapment at the elbow, which is twice as common as personal nerve entrapment at the knee. Radial nerve entrapment at the upper arm and ulnar nerve entrapment in the forearm are much less common.(9)
As detailed earlier, the pathological process leads directly to focal peripherial neuropathy. The basic types of injuries are: laceration, crush, stretch, and rupture. Pressure on the nerve is the primary cause of most damage. Others types include chronic stretching and angulation, repeated stretching and rubbing over a boney surface, tumors, infections, and injections. Irradiation causes fibrosis in and around the nerve resulting in pressure. Exposure to cold is also a basic injury type.
When clients learn that the symptoms they are suffering from have an anatomical basis and that they can be alleviated, it is often the case that they want some dramatic intervention done as soon as possible (e.g., medication, surgery, hypnosis, physical therapy). The problem is that unless there is a significant vascular compromise or motor loss, most cases are best treated initially by conservative methods. (Allopaths treat symptoms that can be verified objectively through standard orthopedic tests. Physicans are reimbursed for performing procedures (e.g., surgery, set broken bones, suture a laceration). Without a diagnosis that requires allopathic intervention of some type, the patient is more often than not referred, with our or without medications, to a physical therapist.)
Neurological Entrapments of the Median Nerve
The median nerve has both motor and sensory fibers; thus, a compromise can cause deficits in both motor and sensory experiences. Most of the sensory issues will be perceived in the palms of the hands, since the vast majority of the sensory fibers terminate in the palm. The motor components innervate the flexors of the fingers and wrists, as well as a number of muscles of the thumb. Weakness and atrophy are the most observable signs of entrapment affecting the motor fibers.(10)
Thoracic Outlet Syndrome
One of the specific entrapmens of the median nerve is thoracic outlet syndrome (TOS). This pattern encompasses a group of maladies that involve the neruovascular structures in the lower parts of the anterior and middle scalene muscles, the first rib, the apex of the lung, the clavical, the brachial plexus, and the subclavian artery and vein. There are three classifications of TOS: vascular TOS can be either venous or arterial; neurologic TOS can be either “true TOS” (classic) or “nonspecific”; neurovascular TOS can be either “traumatic” or “nonspecific.”(11)
In formal or true TOS, there are three primary regions to pay attention to early in the examination: the interscalene triangle, the costoclavicular space, and the pectoralis minor muscle insertion on the coracoid process. In arterial TOS, swelling of the fingers or hand is apparent as a result of poststenotic dialation of the subclavian artery. Venous TOS can be either acute or chronic. It presents with swelling of the arm due to restriction of the subclavian vein.(12)
When suspecting neurogenic phenomenon, or true TOS, first exculpate the neck, specifically the nerve roots of C5 throughT1, looking for myofascial contracture patterns, as well as reports on disc issues, boney spurs, or other growths that could produce pressure on the nerve root.
When cervicogenic issues have ruled out (exculpated), look at the primary locations of entrapment in this syndrome. The site to palpate is at the transverse processes of C7, often called the site of the cervical rib. This is where the elongation of the process becomes a catch point for the brachial plexus and the median nerve.
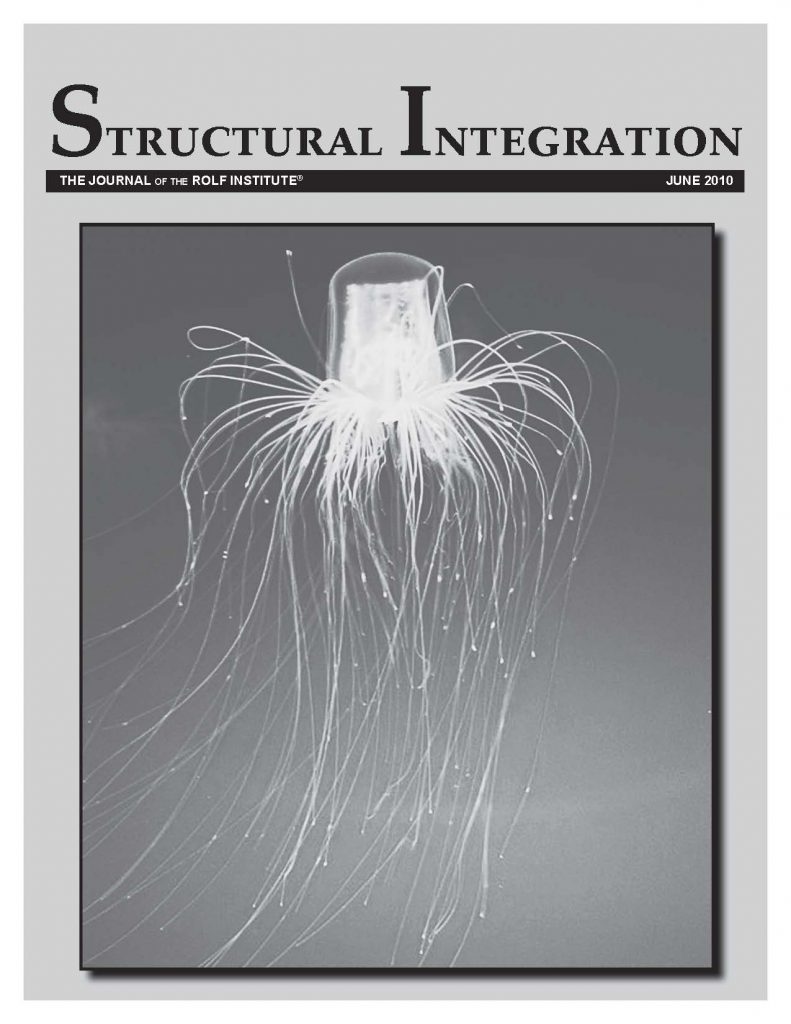
The next structure to look at is the anterior scalene muscle (see Figure 1). When contracted, it is possible for it to put enough pressure posteriorly towards the medial scalene to compress the median nerve between the muscles. From there, follow the nerve under the clavicle, as ptosis of the clavicle can sometimes entrap the nerve and against the first rib, a set of conditions often referred to as the “costoclavicular entrapment syndrome.”(13)
<img src=’https://novo.pedroprado.com.br/imgs/2010/1091-1.jpg’>
Figure 1: Anatomy of the thoracic outlet. A – right anterior view showing nerve and artery passage through the interscalene triangle formed my anterior and medial scalene and first thoracic rib. B – the arrow shows a cervical rib attaching to the upper survace of the first thoracic rib, causing stenosis and poststenotic dilation of the subclavian artery (arterial TOS). C – the arrow shows a fibrous band, arising from the end of a rudimentary cervical rib and attaching to the upper surface of the first thoracic rib, that stretches and angulates the T1 vertical ramus or the proximal lower trunk of the brachial plexus, causing true neurologic TOS.
Laterally, travel to the pectoralis minor region where the median nerve can be trapped under a myofascial contracture of the pectoralis minor, thus pinned against the rib cage. Distally, at the elbow, the median nerve’s path is between the two heads of the pronator teres muscle – CTS is frequently diagnosed when it is actually “pronator syndrome” (same nerve, but a more proximal entrapment). Palpation will, more often than not, differentially diagnose the issue with a negative Tinnel’s sign. Nocturnal symptoms are rare with this syndrome, setting it apart from true carpal tunnel syndrome.
There can be confusion in the assessment of the common entrapments of the median nerve. Severe CTS and true neurologic TOS both produce wasting of the thenar eminence. Typical screening parameters are that the typical age and gender for true TOS is young to middle-aged females, where elderly men are more likely to develop CTS. Another parameter involves the sensory abnormalities. With true TOS the affected regions are along the medial arm, forearm, and hand, while the median nerve distribution in the hand defines CTS. The last parameter is whether or not there are associated neurological abnormalities in the hand. With CTS there are no abnormalities in the ulnar nerve distribution areas; with true TOS, there is weakness and wasting of the ulnar-innervated intrinsic muscles of the hand.(14)
Many patients have the appropriate diagnostic signs and symptoms but no evidence of an abnormal first rib or abnormally long transverse cervical process, or any others static skeletal anomalies. These patients can often present with poor posture and, in particular, ptosis of the scapula on the involved side. The trapezius muscle is more often than not atrophic and weak, allowing the scapula to drop. Habitually poor posture, or overuse with some occupations of particular muscles, can produce similar changes in the scapula musculature. Anatomically, when the scapula drops, more often than not the clavicle also drops. When this occurs, we see in the postural degeneration the opportunity for the brachial plexus to become compromised between the first rib and the clavicle, as well as between the pectoralis minor and the corocoid process.(15) For clients who are obese, weight reduction helps improve posture and lessen the drag on the shoulder girdle.
Carpal Tunnel Syndrome
True CTS is by far the most common neruological entrapment. Predispositions include occupations that require repetitive movements of the hand and wrist, advancing age, and obesity. The clinical feature of CTS is the reporting of nocturnal pain in the hand and fingers, which will often wake the client and is relieved by shaking the hands. When you ask the client for the location of the pain, he/she reliably indicates the median nerve region of the hand. In the later stages of this syndrome the thenar eminence starts to atrophy.(16)
The major components that occupy the carpal tunnel are nine digital flexor tendons and the median nerve (see Figures 2 and 3). The tunnel is a fixed space. It cannot expand, so if the sheaths around the flexor tendons become inflamed and enlarged, neurological entrapment of the median nerve ensues. When the flexors and extensors are balanced and myofascial contractures are reduced, often so are CTS symptoms as well.
<img src=’https://novo.pedroprado.com.br/imgs/2010/1091-2.jpg’>
Figure 2: Carpal tunnel contents and bordering structures.
<img src=’https://novo.pedroprado.com.br/imgs/2010/1091-3.jpg’>
Figure 3: The cutaneous and motor distribution of the median nerve in the hand.
Tinel’s sign has been found to be 50%-75% accurate in predicting subjects who have been electro diagnostically confirmed with CTS. Traditional nonsurgical treatments range from physician referral (to specialists such as neurologists and neurosurgeons), splinting, steroid injections and nonsteroidal anti-inflammatory drugs (NSAIDS). Initial treatment centers on the cause or exacerbation of the complaint. Splinting is the mainstream of conservative care with 14% reporting lasting relief from symptoms and 58% reporting long-term failure. Steroid injections yielded a 33% improvement average reported in seven studies between 1960 and 1984.(17)
Other conservative management approaches involve altering the ergonomic loads or exposures that create or exacerbate CTS symptoms. Tasks involving excessive wrist flexion, extension or deviation, pinching, fine finger motion, and the use of vibratory tools have been implicated. Job modification, tools involved, job rotation, and workstation modification have all been found beneficial to risk reduction.(18)
Neurological Entrapment of the Dorsal Scapular Nerve(19)
Of the common entrapment syndromes, most health-care workers are not particularly familiar with dorsal scapular entrapment. Yet in considering this syndrome, the important role of the dorsal scapular nerves becomes apparent. A functional understanding of the anatomy will equip practitioners with the primary tools necessary to reducing a number of clients’ suffering (see Figure 4).
<img src=’https://novo.pedroprado.com.br/imgs/2010/1091-4.jpg’>
Figure 4: The dorsal scapular nerve as it pierces the medial scalene.
The existence of anterior scalene syndrome has been accepted based on anatomical evidence and clinical corroboration; it is shown to be a vascular type of syndrome. The scalene medius syndrome is primarily concerned with neurological issues.
The course of this nerve after arising from the superior and anterior aspect of the fifth cervical dorsal root, almost immediately passes directly through the medial scalene muscle. From there it travels inferoposterolaterally to its innervation point on the rhomboid muscle.
The entrapment site is where the nerve passes through the anterior aspect of the medial scalene muscle. When entrapped, the dorsal scapular nerve is “hung-up” at this point, thereby preventing the slack required to compensate for necessary and common head and or arm motions. This leaves a tensed nerve moving against taut muscle fibers, which can initiate mechanical irritation in the nerve for a neuropathy.
The dorsal scapular nerve is solely a motor nerve; it does not have skin sensory components. The rhomboids and part of the levator scapulae receive their innervations from this nerve. In an active neuropathy, pain is perceived in the scapular region; if the neuropathy is severe enough, there will be atrophy and weakness in this group of muscles.
When the medial scalene is overactive and the dorsal scapular nerve is entrapped via the traction process outlined above, irritation of that nerve occurs and scapular pain is perceived. If there is a cervical rib, whether complete or otherwise, the inferior aspect of the brachial plexus angulates acutely over the rib and pain follows the ulnar nerve trunk distribution.
Any review of the entrapment of the dorsal scapular nerve must include the anomalous or cervical rib. This structure, when present, is a congenital condition, but is usually never an issue until the third or fourth decade when entrapment most often occurs. One explanation that comes up frequently is a degradation of posture. Poor posture is often typified by forward-shoulder syndrome. This condition puts pressure on the base of cervical spine and leads toward forward-head syndrome as well. This dynamic puts anterior pressure on the entire scalene group. Part of what happens here is that the medial scalene while leaning anterior crimps the dorsal scapular nerve at the entry point into the belly of this muscle. Not only is the nerve entrapped at its entrance, but also restricted in function by an overly strained medial scalene. Now add this to the summation of the effects of aging and repeated small trauma and the case for dorsal scapular nerve entrapment is made.
The diagnosis of dorsal scapular entrapment neuropathy is based on the complaint of pain along the medial border of the scapula on the affected side. Often this symptom is accompanied by diffuse ridiculer pain down the lateral aspect of the arm and forearm. If an injury is involved, it is more than likely an indirect force such as a sudden and violent head jarring. Most all patients are over thirty years of age when there is no specific trauma. Onset is more often than not of a gradual nature. Almost always there will be a positive relationship between pain and head position or motion as opposed to arm position.
During the examination the head will often be carried stiffly and sometimes listing to the affected side. Pain will increase when the head is rotated and laterally flexed, either passively or actively. Significant tenderness will be marked over the lower portion of the medial scalene. Pressure in this area will produce an increase in focal pain as well as radiation to the scapula and down the forearm. Placing the client’s hand on top of his/her head will often relieve the pain, assisting in the confirmation in diagnosis.
Neurological Entrapment of the Ulnar Nerve at the Elbow
Because of it position in the cubital tunnel, the ulnar nerve is very vulnerable to a repetitive traction- and tension-induced stress pattern known as cubital tunnel syndrome.(20) Staal, et al. state that studies have shown that 16% of the general population suffer from a recurrent displacement of the ulnar nerve. They explain that when the elbow is flexed and exteded repetitively a destructive cycle begins: stress, injury, inflammation, and adhesions leading to progressive compressive neuropathy.
Common eitiologys include habitually sleeping with the elbow flexed, work-related repetitive flexion/extension, and over-stretching the arm in catching oneself while falling. Congenital predispositions may increase the probablility of incurring this insult.
Clients with ulnar neuropathy at the elbow often present with paresthesia and pain in the ulnar nerve distribution pattern of the little finger and the lateral aspect of the ring finger.(21) Symptoms are often without regard to origin of this condition (that is, clients may have subjective complaints that are not easily explained by the diagnosis of ulnar neuropathy but can often be directly related) and include an intermittent pattern of numbness and tingling of the outer two digits. As the malady increases in severity, it will generally exacerbate the level of objective finding as well as subjective reporting. Simple elbow flexion will aggrivate all of the symptoms.(22)
Neurological Entrapment of the Sciatic Nerve
Lower back pain coupled with lower extremity pain is one of the most commonly reported neruological syndromes. Sites of compression of the sciatic nerve include the pelvis, the glutei region, and the posterior aspect of the thigh. The most common entrapment site is the glutei region, because the nerve is relatively exposed there. It is possible to compress the nerve by sitting for protracted periods of time on hard or angular surfaces or in peculiar/unusual positions.
Staal, et al.(23) found that a number of different scenarios of prolonged compression in this region could elicit neurological symptoms, such as sitting in an alcoholic and/or drug-induced stupor on the toilet, poor positioning during an anaesthesized surgical procedure, falling asleep in a crossed-legged posture. There is even evidence of what is called “backpocket sciatica” from sitting on an overstuffed wallet.
Piriforms Syndrome
The sciatic nerve passes through the greater sciatic notch, sometimes called the “Gibraltar of the gluteus” along with the performs muscle. The performs muscle has been shown to be comprised of two bellies in almost 20% of the population; in up to 50% of the population, a synovial bursa exists between the performs tendon and the bony material of the sciatic notch. There is also, a lot of variation in the size of this muscle. Obviously, hypertrophy of the performs muscle will result in a reduction of space in the notch, increasing the risk for sciatic nerve compression. Numerous studies have shown that the bifurcation point of the sciatic nerve into its common personal and tibial branches can occur all along its path from the sciatic notch to the popliteal fossa, with 28% bifurcating near the lesser trochanter and 39% just above the popliteal fossa.(24) Of interest here is the fact that this bifurcation can occur before the nerve reaches the performs muscle: in 12% of the population, the personal nerve component passes through the performs, and in a trace amount of cases it passes over the muscle. Thus, the vast majority of the time (87%), the sciatic nerve passes inferior to the performs.(25)
A firm diagnosis of performs syndrome should be arrived at only after there have been strong objective signs that the sciatic nerve is involved and not just glutei pain. The patient will usually present with lumbar-based ridiculer symptoms but without low back pain. When there is a low back pain complaint, more often than not you are dealing with an L5-S1 ridiculer complaint or discogenic referred pain.(26) In performs syndrome cases there is more often more involvement of the personal nerve than the tibial. Complaints will be along the path of the sciatic nerve, there will be deep glutei pain, and internal rotation of the femur will result in exacerbated focal glutei pain as well as paresthesia along top of lower leg and/or foot. The pain complaints are exacerbated with sitting or walking, and lessen when lying supine. Other differentiating symptoms and signs are that there will be no pain in the lumbosacral region. There will be a peripheral instead of ridiculer nerve distribution pattern. The performs will be painful to palpate. Lastly, external femoral rotation will reduce the pain complaint.(27)
Peroneal Entrapment Syndrom
A common entrapment in the lower leg is the personal nerve being compromised in the region of the popliteal fossa and the promixal head of the fibula. This nerve may also be compressed as it winds around the proximal neck of the fibula held against the bone in a fibrous tunnel (see Figure 5). This is a common occurance when one sits with one thigh crossed over the other.(28)
<img src=’https://novo.pedroprado.com.br/imgs/2010/1091-5.jpg’>
Figure 5: Compression of the common personal nerve by the peroneus longus tendon involves both the superficial and deep personal branches.
Frequently, a simple contusion or a chronic compression of the personal nerve against the fibular head will set up this entrapment syndrome. A common phenomenon in motor vehicle collisions is where the lateral aspect of the knee comes into hard contact with either the door panel or the center console of the vehicle. A situation where the knee is resting against one of these vehicle components for period of time will result in compression of the personal nerve and perhaps only a transient syndome instead of chronic.(29)
Assessment of this condition will be from a reporting of either motor or sensory deficits by the client. Examination may reveal a foot-drop condition. Either the deep or superficial branches may be involved in the compression. If there are complaints in the region between the toes, the deep branch is implicated. If there is only paresthesia in or about the lateral aspect of the lower leg, suspect the superficial branch of the personal nerve. In severe cases, there may be radiation up to the sciatic axis.(30)
Conclusion
In my effort to expose Rolfers to various topics in pain management, I spoken at two annual meetings of the Rolf Institute, printed two booklets, and published several articles in Rolf Liines (now Structural Integration). Here I am again.
The vast majority of Rolfers work on issues of pain every day of their practice. Many of the referrals for Rolfing Structural Integration are based specifically on a search for pain relief. Very few clients approach the work for the improvement of their posture alone. Training at the various structural integration schools is extensive. Before a practitioner can bring a “random body” out of chaos and into a more ordered state in gravity, he/she must be well-trained. Further extensive training is required when one is involved in pain management work. There is no question on this matter in reference to osteopaths, naturopaths, or allopaths: extensive training is the most important prerequisite to treating. A Rolfer working on clients’ pain issues without formal and appropriate training specifically in pain management makes it easier for the client to adapt distortion more permanently. It also seriously increases the possibility of mistreating or delaying appropriate treatment for a client in need.
The primary problem with neruological entrapment is not in the treatment but in the assessment or diagnosis. What is important is taking the history and detailing the findings of the examination. Therefore the assessment process is a process of exclusions. The client’s own words and description of his/her complaint and suffering are critical. What type of pain is he/she describing? Where is it? What exacerbates or ameliorates the complaint? A careful examination of muscle weakness (through tests such as heel walking, toe walking, medial and ulnar nerve testing) is very important in finding out what has gone wrong and what direction treatment should take. For those who are obese, weight reduction helps improve posture and lesson the drag on the entire structure.
Initially, the treatment plan should utilize passive modalities and stretching daily for the first week, tapering to three times a week for the next three to six weeks. At that point, a follow up physical examination should indicate a change to active exercising. This regime should be continued until no further improvement is seen and a plateau reached for a few weeks.
Treatment, in the pain management of biomechanical issues, should focus on symptom control. Two aspects of the condition have to be addressed. First, increase the space in the entrapment region and reduce the neurovascular compression. Second – and probably most important _– correct the postural faults and poor body mechanics contributing the condition. This is achieved through manual therapy to include manipulations and mobilization emphasizing stretching and strengthening of the compromised biomechanical system components.
An extensive allopathic approach to postural impacts on neurological entrapments and ideas of correction is detailed in Allieu and Mackinnon’s Nerve Compression Syndromes of the Upper Limb.(31) Approaches from a Rolfer’s perspective, including interventions in the context of the Rolfing ten-session series, are formally addressed in the author’s earlier works.(32, 33) (A bibliography of the author’s writing also appears below.)
Endnotes
Treatment. London: W. B. Saunders, 1999, 1:1-2.
Clay Cox Bibliography
Common Peripheral Nerve Entrapments and Syndromes[:]
To have full access to the content of this article you need to be registered on the site. Sign up or Register.